
Mini-invasive temporalis muscle tendon transfer and lengthening temporalis myoplasty for facial reanimation – a retrospective outcome analysis
Authors:
J. Macek 1; N. Dubovská 1; K. C. Bayezid 1,2; L. Streit 1,2
Authors place of work:
Department of Burns and Plastic Surgery, Faculty of Medicine, Masaryk University, Brno, and University Hospital Brno, Czech Republic
1; Department of Plastic and Aesthetic Surgery, Faculty of Medicine, Masaryk University, Brno, and St. Anne’s University Hospital in Brno, Czech Republic
2
Published in the journal:
ACTA CHIRURGIAE PLASTICAE, 67, 2, 2025, pp. 82-91
doi:
https://doi.org/10.48095/ccachp202582
Introduction
Long-standing facial nerve paralysis profoundly affects patients’ lives [1,2]. This impairment impacts both functional and aesthetic aspects, influencing essential functions such as non-verbal communication, eating [3], drinking, and blinking [4], and can, in some cases, impair nasal breathing. Beyond these physical challenges, facial nerve paralysis also affects social interactions and psychological well - -being [2,5], leading to a substantial reduction in patients’ quality of life (QOL) [6–8].
Local muscle transfers are dynamic procedures used to reanimate the paralysed face. This was first performed by Gilles in 1936 [9], who used an inverted upper part of the temporalis muscle in combination with fascia lata graft for smile reanimation. McLaughin improved this technique in 1943 [10], performing osteotomy of the coronoid process from an intraoral approach and elongation of the temporalis muscle tendon by fascia lata graft to reach the mouth corner. Labbé et al. improved this technique further in 1996 with his version 1 (V1) lengthening temporalis myoplasty (LTM) [11,12] which included mobilisation of the temporalis muscle and tendon transposition to the corner of the mouth. Labbé further improved this technique and in 2009 published version 2 (V2) of lengthening temporalis myoplasty [13] which avoided the osteotomy of the zygomatic arc. Boahene et al. [14] took a different approach to the McLaughins technique. The mini-invasive temporalis tendon transposition (MTTT) includes performing osteotomy of the coronoid process mini-invasively from the nasolabial fold through buccal space, suturing it to zygomaticus major muscle and using a fascia lata strip to reanimate the corner of the mouth.
The alternative dynamic reanimation procedures are free functional muscle transfers pioneered by Hari et al. [15] and Terzi et al. [16] in 1976 and 1997, respectively. These procedures grant more possibilities to the operating surgeon such as a choice of the donor nerve for spontaneous movement of the face or multi-vectoral muscle transfer for a more precise reanimation of the face. However, these procedures are much more complex resulting in longer, often multi-step procedures and higher risk of failure which might not be acceptable for every patient.
As for the evaluation of the reanimation procedures, clinician-graded instruments such as the House-Brackmann score [17], Sunnybrook score [18] or the newer eFACE [19] remain the gold standard. However, QOL-focused questionnaires are getting much recognition in facial reanimation outcome evaluation. The questionnaires used include the SF-36 [20], FACE [21] and the FPD questionnaire, which was developed by our senior author.
In this article, we introduce a retrospective study of the management of facial palsy patients by LTM or MTTT procedures as well as our method of outcome evaluation based on both patient and clinician-reported tools in 23 flaccid facial palsy patients operated on at the Department of Plastic and Aesthetic Surgery, St. Anne’s University Hospital in Brno.

Patients and methods
Patient cohort
This study included 23 patients with long-standing flaccid facial palsy (duration > 18 months) who underwent facial reanimation by either LTM (8 patients) or MTTT (15 patients), augmented in some cases by either/both nasal ala suspension or lagophthalmos correction, at the Department of Plastic and Aesthetic Surgery of St. Anne’s University Hospital in Brno between the years 2015 and 2021. All patients provided informed consent, and the study was approved by the institutional ethics committee (approval number: EK-FNUSA/2023).
Patient groups according to surgical method
Two primary local muscle transfer techniques were used for dynamic smile reanimation. Patients were retrospectively assigned to one of two study groups according to the reanimation method they had undergone.
Lengthening temporalis myoplasty group (LTM group)
The first technique was a slightly modified lengthening temporalis myoplasty (V2), originally described by Labbé in 2009 [13]. This method was performed using two incisions: a coronal incision and a nasolabial fold incision. Through the coronal incision, the posterior half of the temporalis muscle was detached in the subgaleal plane. The coronoid process was transected via the nasolabial incision, and the temporalis tendon was advanced and affixed to the upper lip (Fig. 1).

Minimally invasive temporalis tendon transfer group (MTTT group)
The second technique used was a mini-invasive temporalis muscle tendon transfer introduced by Boahene et al. in 2011 [14]. The procedure was performed through a single nasolabial incision. The coronoid process was accessed through the buccal space and osteotomized. The tendon of the temporalis muscle was advanced toward the lip and was extended with a fascia lata graft, as the tendon alone was not found to be of sufficient length (Fig. 2).
Procedures performed in both groups
These dynamic procedures were combined with adjunctive static procedures to address other disabilities of the patient utilizing the concept of graduated minimally invasive facial reanimation. Specifically, nasal ala suspension and lagophthalmos correction were performed, either simultaneously or in a staged approach.
The nasal ala suspension was performed through a short preauricular incision. A fascia lata strip, 8–10 mm in width, was tunnelled in the sub-SMAS plane and anchored to the deep dermis at the level of the nasal ala. Adequate tension was applied to reopen the nasal passage, and the strip was then secured to the SMAS and/or parotid fascia at the preauricular site.
Lagophthalmos correction of the lower eyelid was performed using a technique modified by the senior author, based on the method originally described by Prof. Dr. M. Frey, involving a 2–3 mm-wide strip of either palmaris longus tendon or fascia lata. The incision was made in the medial canthus to expose the medial canthal ligament. The graft was inserted from the lateral canthus through a tunnel above the tarsal plate, using a fine liposuction cannula, and affixed to the medial canthal ligament (using either stitches or slipknot). Two adjacent drill holes were created approximately 1 cm above the lateral incision to the orbital rim, and the lateral end of the graft was anchored at this site.
Post-operative physiotherapy
Postoperative rehabilitation was considered essential in optimizing outcomes following local muscle transfer. It was aimed at improving muscle tone, increasing the range of motion, and enabling patients to develop voluntary and, potentially, spontaneous smiling.
The Mirror-Effect Protocol, developed by Blanchin and Labbé in 2013, was implemented. A smartphone application was used to digitally mirror the healthy side of the face and replace the paralyzed hemiface in real time. Patients were instructed to practice smiling while receiving visual feedback from the app and tactile feedback by touching the reanimated side of the face. This approach was intended to stimulate neuroplasticity and was found to support improved voluntary control of the reanimated hemiface.
Outcome evaluation
Every patient at our clinic undergoes pre and post-operative evaluation by clinician-reported instruments eFACE and House-Brackmann score as well as self-reported FPDQ to determine both objective and subjective changes in patient’s status.
Each patient was assessed both preoperatively and postoperatively using standardized clinician-reported and patient-reported outcome measures. Clinician-reported assessments included the eFACE scale and the House-Brackmann (HB) grading system. Patient-reported outcomes were evaluated using FPDQ, a validated 30-item instrument developed by the senior author to assess QOL changes in patients undergoing facial reanimation. The questionnaire is subdivided into sections focusing on eye problems (FPD-S-EYE), face and mouth problems (FPD-S-FACE), social life implications (FPD-S-SOCIAL) and evaluation of synkinesis (FPD-S-SYNK). Each section is evaluated individually, and all of the sub-scores combine to give an overall score (FPD-S).
Statistical analysis
All statistical analyses were conducted by the Institute of Biostatistics and Analyses, Ltd., using IBM SPSS software (version 24). Changes in continuous variables between preoperative and postoperative values were evaluated using the Wilcoxon signed-rank test. Differences in categorical variables, such as HB score, were analysed using Fisher’s exact test. A P-value < 0.05 was considered statistically significant.
Results
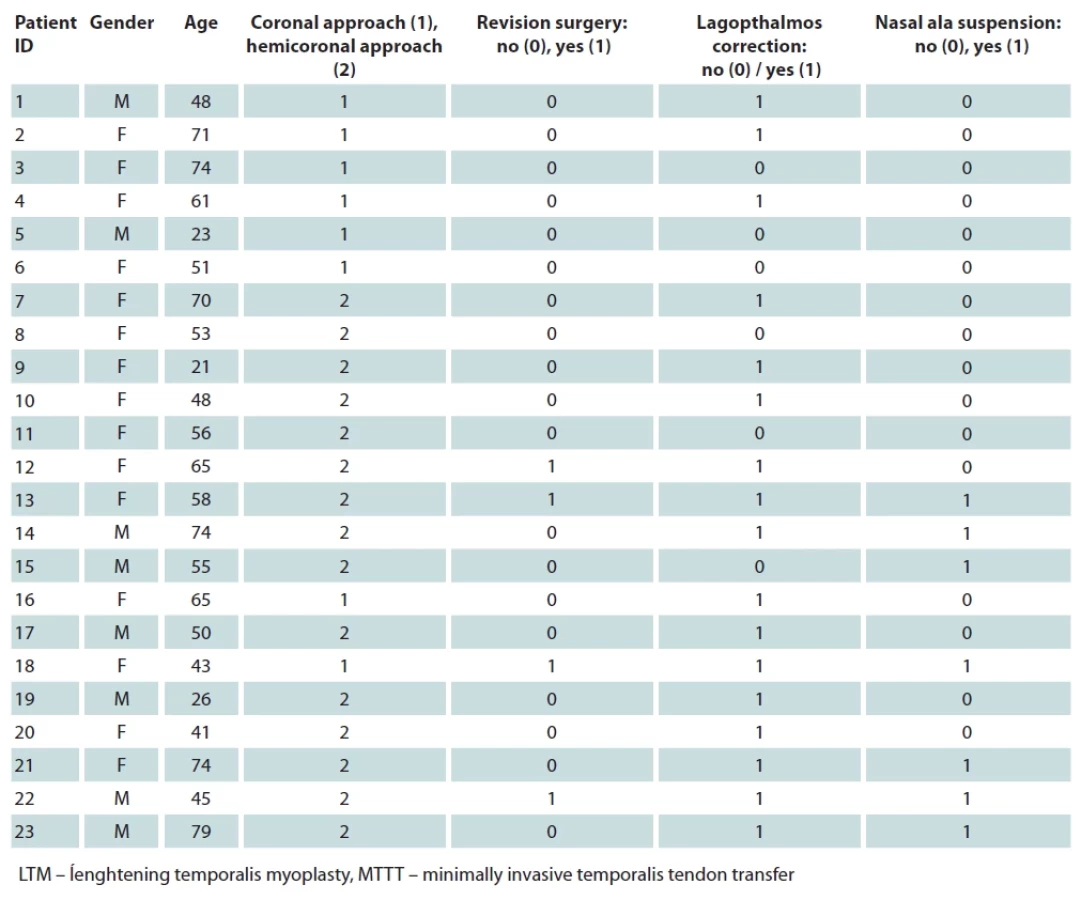
The mean age of the patients was 54.4 years (SD = 16.1). There were 15 female and 8 male patients. In some patients, the dynamic reanimation procedure was supplemented by nasal ala suspension (7 patients) and/or lagophthalmos correction (17 patients). A detailed breakdown of the patient group is presented in Tab. 1. All patients agreed for their anonymized data to be used for research purposes.
All patients achieved a stable result after the local muscle transfer surgery in 10.6 (SD = 7.8) months. The mean improvement in clinician-graded tools was 1.6 points (SD = 0.6) in HB score and 31.7% (SD = 15.8) in eFACE static score and 29.9% (SD = 18.2) in eFACE dynamic score, respectively. For the patient-reported measurement, the overall score (FPD-S) improved by 31.4% (SD = 13.2) Revision surgery was required in four cases. The reanimation results of the whole patient group are summarized in Tab. 2.
In MITTT group (N = 14), the mean improvement in clinician-graded tools was 1.6 points (SD = 0.5) in HB score and 34.1% (SD = 14.1) in eFACE static score and 28.1% (SD = 19.0) in eFACE dynamic score, respectively. For the patient-reported measurement, the FPD-S score improved by 34.2% (SD = 11.3). The reanimation results of the MTTT group are summarized in Tab. 3. Out of these patients, six have the procedure modified by lagophthalmos correction and six by lagophthalmos correction and nasal ala suspension. Revision surgery was required in three cases due to over correction of the oral commissure position. The revision surgery consisted of adhesiolysis of the graft from the nasolabial incision and prolonging the length of the graft (in the primary procedure the graft is affixed to SMAS to leave approx. 1 cm in reserve). Representative clinical photographs before and after temporal myoplasty are shown in Fig. 3.
Patients who underwent LTM procedure (N = 8) achieved a mean improvement in clinician-graded tools of 1.6 points (SD = 0.7) in HB score and 27.4% (SD = 14.1) in eFACE static score and 33.3% (SD = 17.2) in eFACE dynamic score, respectively. For the patient-reported measurement, the FPD-S score improved by 26.2% (SD = 15.7). The reanimation results of the whole patient group are summarized in Tab. 4. Out of these patients, four of them have the procedure modified by lagophthalmos correction and one of them by lagophthalmos correction and nasal ala suspension. Revision surgery was required in one case also due to over correction of the oral commissure position. The revision procedure, also performed from the nasolabial fold incision, prolonged the graft using a reserved length of the temporalis muscle tendon. Representative clinical photographs before and after temporal myoplasty are shown in Fig. 4.
No statistically significant differences were found between the outcomes of the two groups. Comparison of the LTM and MTTT groups is shown in Graph 1 for eFACE and FPDQ and in Graph 2 for HB score.







Discussion
Patients with long-standing flaccid facial paralysis (> 18 months) may benefit from surgical facial reanimation. Dynamic smile restoration procedures – either local muscle transfer or free functional muscle transfer – are considered standard and effective treatment options. These are generally recommended in combination with individualized static procedures, in accordance with the concept of graduated minimally invasive facial reanimation [22].
The aim of this study was to retrospectively compare two temporalis muscle-based facial reanimation techniques – the lengthening temporalis myoplasty [13] and the minimally invasive temporalis tendon transfer [14] – in an institutional cohort of patients. Both techniques were initially implemented in the senior author’s surgical practice and subsequently refined throughout the study cohort, with minor modifications introduced over time as experience with each approach increased. All patients included in the study, regardless of group assignment, achieved a stable clinical outcome in terms of dynamic facial reanimation. There was a statistically significant improvement in both the patient-reported outcome measure (FPDQ) and the clinician-graded assessments (HB score and eFACE), indicating that both techniques, as performed in our practice, appear to be safe and effective treatment options. When comparing the two techniques (LTM vs. MTTT), no statistically significant differences in these parameters were observed between the outcomes of the two patient groups. Comparison of LTM/MTTT outcomes are lacking in current literature. Although a study by House et al. [23] have addressed facial reanimation using both LTM/MTTT, it lacks specific comparison of the outcomes of the two techniques,
Given these findings, assessment of donor-site morbidity and complications – particularly those leading to secondary surgeries – may be equally or even more important in distinguishing the overall impact of each method on patient care and guiding treatment selection. Based on the available literature, direct comparison of complications between LTM (V2) and the Boahene technique of MITTT remains limited in the current literature. While both techniques aim to restore dynamic facial function in patients with facial paralysis, studies often focus on single-method case series or small cohorts, with varying definitions and reporting of complications.
Donor-site morbidity is an important consideration when comparing MTTT and LTM techniques. In the MTTT procedure, fascia lata is often harvested to extend the temporalis tendon, which can result in thigh-related complications such as postoperative pain, local swelling, hematoma, and, in some cases, patient-reported discomfort during ambulation or long-term bulking at the donor site. On the other hand, fascia lata graft can be advantageously used simultaneously for nasal ala suspension/ lagophthalmos correction without any additional donor site morbidity.
In contrast, the LTM technique typically requires the coronal incision, which, although offering good exposure, carries the risk of temporal hollowing due to muscle mobilization, as well as potential scar-related concerns and alopecia along the incision line. Moreover, if LTM is combined with any static suspension techniques, additional donor-site morbidity may result from the harvesting of palmaris longus tendon or fascia lata grafts, commonly used in these procedures.
While both donor sites are generally well tolerated, these different morbidity profiles may influence surgical decision-making, particularly in younger patients or those with aesthetic concerns.
Another consideration is the risk of nasolabial fold overcorrection in the resting position, potentially caused by retraction of the undetached temporalis muscle. For these reasons, and as a preventive measure, the detached insertion of the temporalis muscle is first anchored to the SMAS in the nasolabial region during the LTM procedure. Only then is the position of the nasolabial fold precisely balanced using adaptive sutures, which secure the released temporalis muscle to the anterior edge of the temporal fossa, in order to minimize the risk of temporal hollowing. Additionally, percutaneous intraoperative electrical stimulation has been described as a method for adjusting the position of the nasolabial fold [24]. In our study, a higher rate of revision surgery to address nasolabial fold overcorrection at rest was observed in the MTTT group (20% of patients) compared to the LTM group (12.5%); notably, no intraoperative electrical stimulation was employed in any of the cases.
Furthermore, the formation of adhesions within the buccal space may represent a postoperative complication that can restrict smile excursion and limit functional outcomes. Distal transposition of the temporalis muscle into the buccal space may be considered a potential advantage of the LTM technique, as it positions the motor unit closer to the site of movement. As a result, the final excursion of the smile may be less restricted compared to the MTTT approach, where the use of tendon or fascial grafts can be associated with a higher risk of adhesion formation in the postoperative course. However, due to the limited number of patients in our cohort as well as lack of oral commissure excursion data we are unable to comprehensively prove this claim.
At our study cohort, LTM and MTTT procedures were recommended especially for patients with higher biological age and/or comorbidities due to shorter operating time comparing with free functional muscle transfer, smaller risk of complications and surgical revision. It was also advisable for patients wanting less extensive surgery with immediate results and simpler physical therapy. We also recommended local muscle transfer for patients with decreased facial nerve function on the “healthy” side as it contraindicates the use of cross-facial nerve graft for achieving spontaneous smile with free functional muscle transfer. The weakness of the “healthy” side can be examined clinically and confirmed using an EMG measurement of mimic muscles.
In our study cohort, the LTM and MTTT procedures were primarily recommended for patients of advanced biological age and/or with significant comorbidities, due to their shorter operative time, lower risk of complications, and reduced need for surgical revision potentially associated with free functional muscle transfer (FFMT). These approaches were also considered suitable for patients preferring less extensive surgery with immediate functional results and a simpler rehabilitation process. Furthermore, local muscle transfer was favoured in patients with reduced facial nerve function on the contralateral (‘healthy’) side, which contraindicates the use of cross-facial nerve grafting required for spontaneous smile restoration in FFMT. Weakness on the unaffected side was assessed clinically and confirmed via electromyographic (EMG) evaluation of the mimetic muscles.
The study is limited by the relatively low number of patients (23 in total) included in the study. Furthermore, the differing sizes of the two groups might have skewed the data. The mean age of the patient group (54.4 years) is relatively high. However, this is due to the fact, that we generally recommend local muscle transfers to patients with higher biological age.
Systematic and statistically meaningful comparison of surgical techniques is further complicated by the high variability in the clinical presentation of facial paralysis, as each patient presents with a unique set of impairments. This further implicates the need for an individualized, modular approach to the treatment of facial paralysis and thorough evaluation of the patient (clinical examination, QOL implications evaluation, objective evaluation of the paralysis) to provide patients with the best outcomes possible. We are looking forward to reevaluating our treatment algorithm based on data from more patients.
Conclusions
Both temporalis muscle–based facial reanimation techniques compared in our patient cohort – LTM and MTTT – were shown to be reliable treatment options for long-standing flaccid facial paralysis. A statistically significant improvement was observed in both patient-reported outcomes (FPDQ) and clinician-graded assessments (House-Brackmann score and eFACE) in each group when compared to preoperative status. However, no statistically significant differences were found between the LTM and MTTT groups in these parameters, suggesting that other factors, such as complication rates, donor-site morbidity, and surgical extent, should be considered when choosing a preferred technique. A limitation of this study is the relatively small number of patients in each group, highlighting the need for prospective and/or multicentric studies to validate and confirm our findings.
Roles of authors
The surgeries were performed by our corresponding author, Assoc. Prof. Libor Streit MD., PhD., as well as study conceptualization, supervision and final approval of the manuscript. Nikola Dubovská, MD led patient data collection, analysis and evaluation. K. Can Bayezid, MD participated in data analysis and evaluation. Jan Macek performed the literature review and original draft preparation. He also participated in the data analysis, evaluation and interpretation.
Disclosure
The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. This study was approved by the institutional ethics committee of St. Anne’s University Hospital in Brno (approval number: EK-FNUSA/2023) and was conducted according to the tenets of the Helsinki Declaration.
Zdroje
Department of Burns and Plastic Surgery
Faculty of Medicine, Masaryk University
Jihlavská 340/20
625 00 Brno
Czech Republic
libor.streit@med.muni.cz
Accepted: 5. 7. 2025
Štítky
Chirurgia plastická Ortopédia Popáleninová medicína TraumatológiaČlánok vyšiel v časopise
Acta chirurgiae plasticae
2025 Číslo 2
- Liečba bolesti po jednodňovej chirurgii
- Fixní kombinace tramadol/paracetamol je doporučenou volbou v léčbě chronické bolesti v ordinaci praktického lékaře
- Kombinace kodein/paracetamol prokázala stejný analgetický účinek jako hydrokodon/paracetamol
- Nová metoda kombinované analgetické léčby vychází z multimechanistické povahy bolesti
- Léčba chronické bolesti u starších pacientů vychází z farmakologických i nefarmakologických přístupů
Najčítanejšie v tomto čísle
- Mini-invasive temporalis muscle tendon transfer and lengthening temporalis myoplasty for facial reanimation – a retrospective outcome analysis
- Limb saving with regenerative medicine tactics – a case report
- Risk factors for cleft lip and palate in the Czech population – a double center study
- Surgical management of accessory breast tissue: liposuction and mastectomy in axillary localization – a case series