
Limb saving with regenerative medicine tactics – a case report
Authors:
F. Contoli Isoldi; L. Vieites; A. K. De Sá Reis; L. M. Ferreira
Authors place of work:
Plastic Surgery Division / Surgery Department, Universidade Federal de São Paulo, São Paulo, Brazil
Published in the journal:
ACTA CHIRURGIAE PLASTICAE, 67, 2, 2025, pp. 111-115
doi:
https://doi.org/10.48095/ccachp2025111
Introduction
Regenerative medicine has gained significant attention due to its wide range of strategies for tissue restoration and restructuring. This therapeutic approach combines knowledge from cellular biology, tissue engineering, and translational medicine, providing new hope for the treatment of conditions that previously lacked definitive therapeutic options [1–3].
Although tissue regeneration occurs naturally in our bodies, this process is limited to certain organs, such as the liver, whose hepatocytes have a remarkable capacity for regeneration, and to superficial epidermal injuries, such as first-degree burns, which typically regenerate without leaving scars [4]. Regeneration is characterized by the replacement of damaged cells with the same type of cells, resulting in the complete restoration of tissue structure and function. In contrast, healing is a repair mechanism that, while necessary, often results in scar tissue that may not have the same functional properties as the original tissue.
Given this natural limitation, regenerative medicine presents itself as an innovative approach aimed at enhancing the body’s regenerative capacity. The manipulation of growth factors, such as platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF), has been shown to increase vascularization and cell proliferation, facilitating tissue regeneration in experimental and clinical models [5]. Additionally, the use of biomaterials, such as biocompatible scaffolds, can provide structural and functional support, promoting cell adhesion and differentiation, which is crucial for effective regeneration [6,7]. These interventions can not only accelerate the healing process but also induce a process more akin to tissue regeneration, promoting recovery that approaches the original function of the tissue.
Autologous fat grafting has been widely used as a tool in regenerative medicine, proving effective in promoting tissue regeneration in various clinical situations. This is primarily due to its rich composition of mesenchymal stem cells (MSCs) and growth factors from adipose tissue, which play crucial roles in tissue regeneration. The MSCs present in adipose tissue are known for their ability to differentiate into various cell types and secrete cytokines and growth factors that promote angiogenesis and healing [8]. Growth factors, such as PDGF and VEGF, are released during the grafting process, stimulating the formation of new blood vessels and cell proliferation, which is essential for effective tissue regeneration [9]. Furthermore, the interaction between stem cells and tissue microenvironments favors inflammation modulation and promotes healing, resulting in a more efficient and functional recovery [10]. These mechanisms contribute to the fact that fat grafting not only fills tissue defects but also actively participates in the regeneration and restoration of the original functions of the tissue.
Case studies demonstrate that lipografting can improve wound healing in patients with chronic ulcer, as evidenced by a series of cases in which autologous fat grafting led to a significant reduction in the dimensions of lesions and an increase in local vascularization [9]. Numerous studies have also shown the effectiveness of fat grafting in breast reconstruction for patients who have undergone radiotherapy, where lipografting contributed not only to aesthetics but also to tissue function, reducing fibrosis and improving skin quality [11]. These evidences reinforce the role of fat grafting as a promising strategy for tissue regeneration in various conditions.
The objective of this study is to report a case of limb salvage from amputation using regenerative medicine tactics.
Description of the case
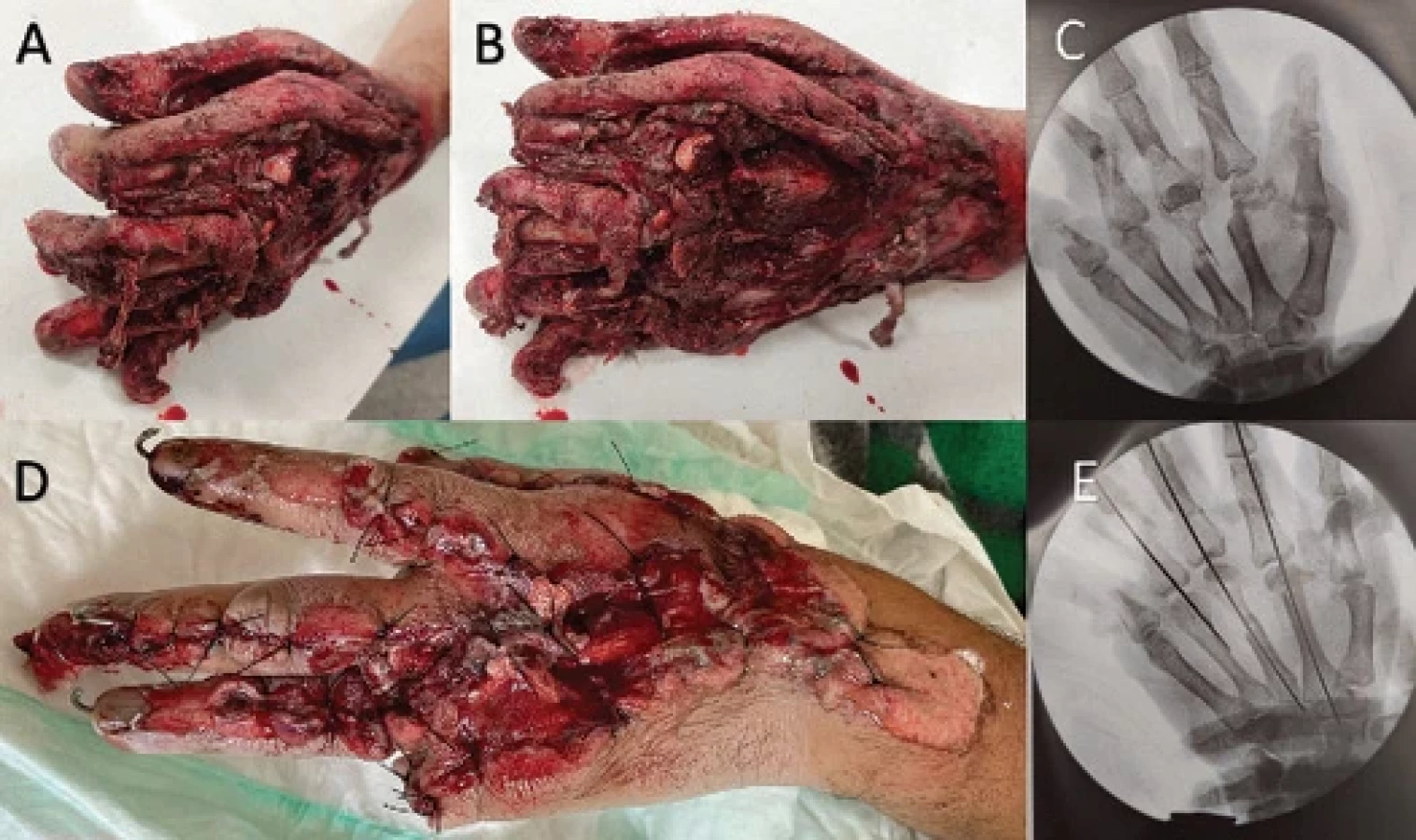
Patient GTM, a 27-year-old male, was involved in a car accident on December 9, 2022, sustaining severe trauma to his left hand, including crushing, degloving, and multiple fractures. Physical examination revealed that the patient retained the ability to move his thumb, allowing for a pinch grip with the other fingers. Despite the complex tissue injury, which could lead to amputation – a reasonable and prudent solution – the decision was made to preserve the limb and engage the plastic surgery team. Necrotic tissue debridement, fracture fixation, and amputation regularization of the fifth finger were performed (Fig. 1) with assistance from the orthopedic team.
Given the complex injury in the distal portion of the limb, with exposure of vital structures and limited therapeutic options for coverage with flaps, treatment with fat grafting was considered to promote tissue regeneration until a future skin graft could be performed.
Every seven days, the patient underwent surgical debridement and lipografting over the wound areas, with the entire hand covered with a negative pressure dressing. A total of four similar procedures were conducted (Fig. 2, 3), showing progressive and gratifying improvement until the fifth week of treatment, when the bed on the dorsum of the hand presented adequate granulation tissue (Fig. 4). At this point, the team performed a thin partial skin graft, with the donor site being the ipsilateral forearm.
The fat used in the treatments was aspirated from the lower abdomen and medial thighs, using a 0.9% saline solution with adrenaline at a concentration of 1 : 250,000. A 3 - mm cannula with three “Mercedes” type holes was used, and negative pressure was applied with a 60 mL syringe. The collected tissue was left in the syringes to settle for approx. 15 min, without contact with ambient air. The liquid fraction was discarded, using only the fat and the supernatant, averaging about 35 mL per application. The lipograft was placed over the granulating wound bed without infiltration into the tissue. All surgical procedures were performed under general anesthesia.
The dressing after each lipografting procedure consisted of rayon gauze, covered with the lipograft supernatant and sterilized petroleum jelly, cotton gauze (Zobec®) on the dorsum of the hand, and gauze between the fingers, wrapped in cling film and maintained under negative pressure at 125 mmHg for seven days.
After five weeks of treatment, a skin graft was performed (Fig. 4), closed with a dressing similar to previous ones, without lipograft and negative pressure. This dressing was opened seven days after the skin graft, and the patient returned for an outpatient visit 14 days post-operation (Fig. 5), showing good skin integration and the beginning of functional conditioning of the limb.




Discussion
The concepts of regenerative medicine are increasingly being applied through its arsenal, such as lipografting. In complex wounds, where there is tissue loss, exposure of vital tissues, and functional deficits, this option serves as a safeguard for recovering, organizing, and restructuring the remaining tissues for the benefit of the critically ill patient. In the case presented, during the initial assessment of the patient by the emergency team, amputation was considered. The patient’s hospital course utilized many resources, both material and human, but the tissue recovery leading to final skin coverage, along with the preservation of the limb, would likely compensate for the functional recovery of the hand and the patient’s return to activities in the medium to long term.
Conclusion
This case report demonstrated success in salvaging a limb from amputation using lipografting, a tactic within the arsenal of Regenerative Medicine. More studies focusing on this approach are necessary to further highlight the benefits of lipografting in the treatment of complex wounds and limb salvage.
Roles of the authors
Substantial contributions to the conception or design of the work – Felipe Contoli Isoldi;
acquisition, analysis, or interpretation of data for the work – Felipe Contoli Isoldi and Ana Karenina de Sá Reis, drafting the work or revising it critically for important intellectual content – Felipe Contoli Isoldi and Luiza Vieites; final approval of the version to be published – all authors; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved – all authors.
Disclosure:
The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Zdroje
Štítky
Chirurgia plastická Ortopédia Popáleninová medicína TraumatológiaČlánok vyšiel v časopise
Acta chirurgiae plasticae
2025 Číslo 2
- Liečba bolesti po jednodňovej chirurgii
- Fixní kombinace tramadol/paracetamol je doporučenou volbou v léčbě chronické bolesti v ordinaci praktického lékaře
- Kombinace kodein/paracetamol prokázala stejný analgetický účinek jako hydrokodon/paracetamol
- Nová metoda kombinované analgetické léčby vychází z multimechanistické povahy bolesti
- Léčba chronické bolesti u starších pacientů vychází z farmakologických i nefarmakologických přístupů
Najčítanejšie v tomto čísle
- Mini-invasive temporalis muscle tendon transfer and lengthening temporalis myoplasty for facial reanimation – a retrospective outcome analysis
- Limb saving with regenerative medicine tactics – a case report
- Risk factors for cleft lip and palate in the Czech population – a double center study
- Surgical management of accessory breast tissue: liposuction and mastectomy in axillary localization – a case series