Functional outcome of peripheral nerve schwannoma – a case series
Authors:
J. K. Mishra 1; A. Valsalan 1; S. A. Sahu 1; M. De 2
Authors place of work:
Department of Burns & Plastic Surgery, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India
1; Department of Burns & Plastic Surgery, All India Institute of Medical Sciences, Guwahati, Assam, India
2
Published in the journal:
ACTA CHIRURGIAE PLASTICAE, 67, 2, 2025, pp. 116-126
doi:
https://doi.org/10.48095/ccachp2025116
Introduction
Schwannomas are benign, usually painless, firm nodules ranging in size from 1 to 2 cm in diameter. They originate from Schwann cells of the peripheral nerve sheaths [1] and account for 8% of soft tissue tumors in the upper extremity [2]. In the upper limb, schwannomas typically affect major nerves along flexor surfaces, such as the ulnar and median nerves, while only 7% of all peripheral schwannomas involve the radial nerve [2]. Most patients are asymptomatic, and malignant potential is low, though rare malignant conversions have been reported. Tumours often present with a tingling sensation, though this is not a consistent clinical finding. Schwannomas tend to grow slowly, and the presence of positive Tinel’s sign and paresthesia can assist in diagnosis.
Imaging studies, such as magnetic resonance imaging (MRI) and ultrasonography [3], are essential for identifying the tumor’s origin and distinguishing schwannomas from other soft tissue tumors, such as ganglions [4]. Histologically, schwannomas feature a highly cellular Antoni A component, with Verocay bodies, and a myxoid, hypocellular Antoni B component [1].
Although there are case reports available regarding schwannoma arising from main radial nerve and median nerve, there are less articles available regarding case series of schwannoma arising from major peripheral nerves
In this article, we discuss a series of peripheral nerve schwannomas which we have managed and their functional outcomes.
This retrospective analysis was conducted at the Department of Burns and Plastic Surgery, All India Institute of Medical Sciences, Raipur, India, over a two-year period from September 2021 to September 2023. We analyzed the functional outcomes following surgical excision of peripheral nerve schwannomas, with a minimum follow-up of 6 months.
Data were collected for each patient, including demographics, age at presentation, initial symptoms, and duration. We reviewed the dates and types of surgeries performed. Preoperative and postoperative functional outcomes were assessed using standardized grading systems. Motor function and muscle strength of the upper and lower limbs were evaluated before and after surgery using the British Medical Research Council (BMRC) grading system (Tab. 1) [5]. Sensory function in the lower limbs was assessed using the Modified Highet Classification (Tab. 2) [6], and in the upper limbs using the BMRC scale modified by Omer and Dellon [7,8]. Both assessments were performed during hospitalization and at the last follow-up.
Tab. 1. British Medical Research Council grading system for motor assessment.
Tab. 2. Modifi ed Highet Classifi cation for sensory assessment.
Description of the case
Case 1
A 30-year-old male, car mechanic by occupation, presented to the outpatient department with a recurrent swelling over the lower lateral aspect of his left arm, associated with pain, tenderness, and tingling sensations extending distally from the swelling. The symptoms had persisted for one year. He had a similar swelling ten years earlier, which had been operated elsewhere, though no records of the previous surgery were available. The patient had no other comorbidities.
On examination, there was a firm, minimally tender, non-pulsatile, non-compressible swelling measuring 5 × 3 cm over the lower third of the lateral aspect of the left arm, just above the lateral condyle. The swelling’s mobility was restricted during elbow flexion against resistance. Tapping over the area caused tingling over the little and ring fingers. Shoulder and elbow movements were normal, and no distal motor deficits or lymphadenopathy were noted. Routine laboratory tests were within normal limits.
Ultrasonography revealed a well-circumscribed hypoechoic lesion with a central anechoic area measuring 3.7 × 2.6 cm, located in the intermuscular plane of the left arm, with mild peripheral vascularity and areas of cystic degeneration. MRI showed an ovoid, well-defined, enhancing lesion in the antecubital region, displacing adjacent muscles, with hemorrhagic and cystic changes, consistent with a nerve sheath tumor – most likely a schwannoma originating from the radial nerve. Fine needle aspiration confirmed the diagnosis, revealing a paucicellular smear with benign-appearing spindle cells against a hemorrhagic background.
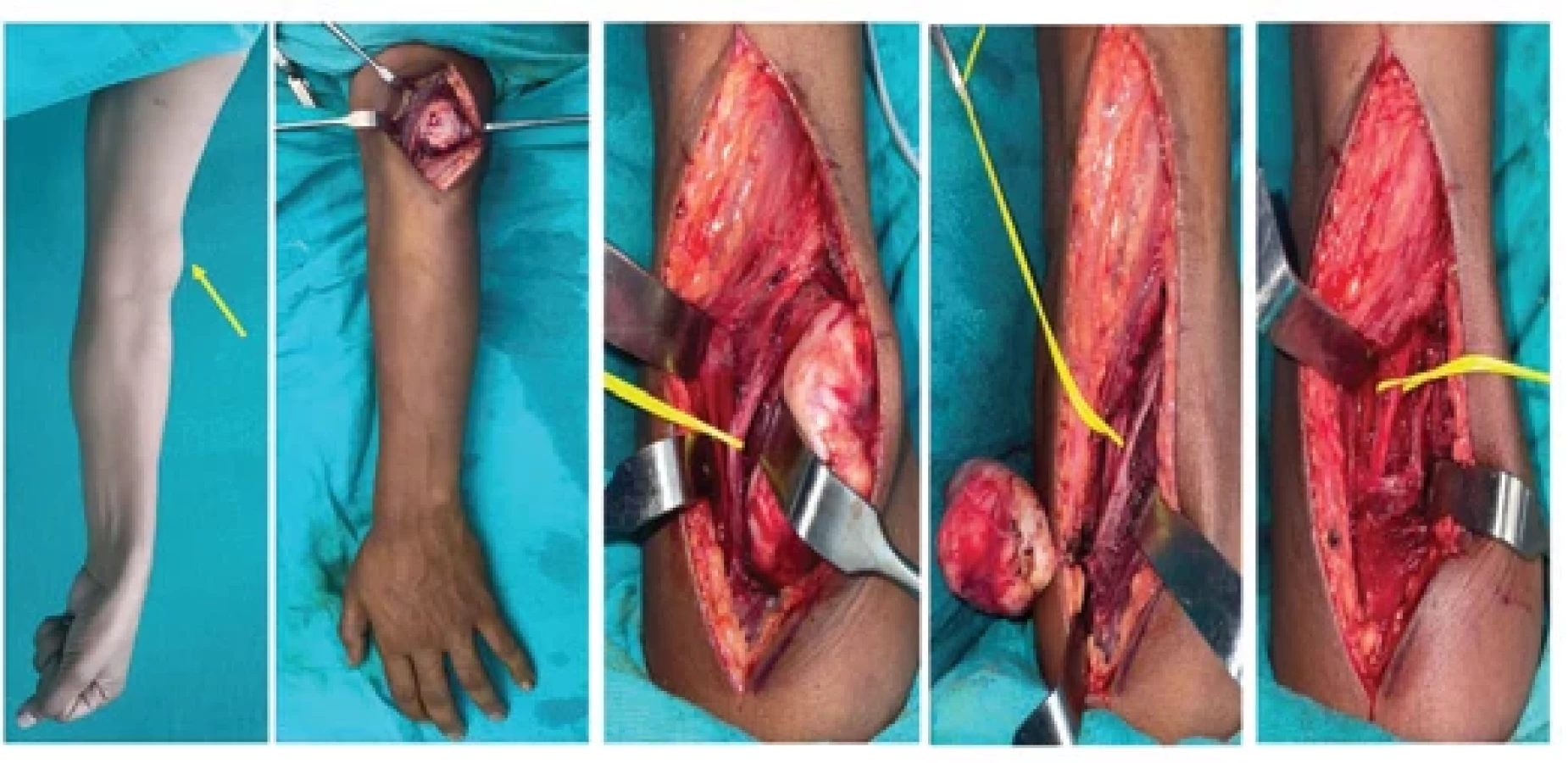
During surgical excision, an encapsulated swelling measuring 5 × 3 cm was noted, encasing the radial nerve in the intermuscular septum. Under loupe magnification, the nerve was carefully dissected from the fascicles. Intraoperative nerve stimulation before and after excision confirmed the continuity of conducting healthy nerve fascicles (Fig. 1).
Histopathological findings suggested a well-encapsulated tumor with hypercellular and hypocellular areas, spindle cells in fascicular arrangements, moderate nuclear pleomorphism, eosinophilic cytoplasm, Verocay bodies, and hemosiderin-laden macrophages with no evidence of necrosis or mitotic activity.
During follow-up, the patient initially experienced mild sensory disturbances along the posterior cutaneous nerve of the forearm, which resolved to S4. No motor deficits were noted, and after one year, the patient remained asymptomatic, with fully preserved radial nerve function.
Fig. 1. Schwannoma arising from the left side main radial nerve; on exploration, it was found to originate from a single fascicle. The tumor was excised preserving the nerve fascicle.
Fig. 2. Schwannoma arising from the left side main radial nerve. The tumor appears encasing one nerve fascicle, which was also removed along with the tumor and nerve continuity was re-established using single sural nerve cable graft.
Case 2
A 55-year-old male office clerk presented to the outpatient department with complaints of swelling in the left arm region, which had been progressively increasing in size over the past four years. The swelling had an insidious onset. The patient was initially evaluated by another department, where an MRI was done which suggested the possibility of a schwannoma arising from the left radial nerve. Core needle biopsy of the swelling showed possible diagnosis of epithelial hemangioendothelioma, and the patient was referred to our center for further management. He reported no associated weakness, numbness, or paresthesia in the left upper limb, and there were no other similar swelling elsewhere on the body.
On local examination, a 7 × 6 cm ill-defined, slightly tender, minimally mobile, soft to firm swelling was observed over the anterolateral aspect of the left arm. The swelling appeared more prominent on elbow flexion, but there was no evidence of distal neurovascular deficits.
Intraoperatively, a 5 × 4 cm well-encapsulated, globular, grey-white swelling was found, originating from a single fascicle of the left radial nerve. During intraoperative nerve stimulation, stimulation of the involved fascicle did not demonstrate wrist or finger extension on the left side. The tumor was found splaying the left brachioradialis muscle. The entire tumor was excised, and the involved fascicle was sacrificed. The nerve was repaired using a single sural nerve graft harvested from the left leg (Fig. 2).
Microscopic examination of the swelling showed a well-encapsulated tumor composed of both hypocellular and hypercellular areas. The tumor consisted of elongated spindle-shaped cells with tapering ends, vesicular nuclei, occasional prominent nucleoli, and a moderate amount of eosinophilic cytoplasm, along with Verocay body formation. Multiple areas of dilated cystic spaces and hemorrhage were noted, as well as hyalinized blood vessels and melanin pigment deposits, suggesting a diagnosis of ancient schwannoma (Fig. 3) and immunohistochemistry of the swelling showed positivity for CD34, EMA, S100 (Fig. 4).
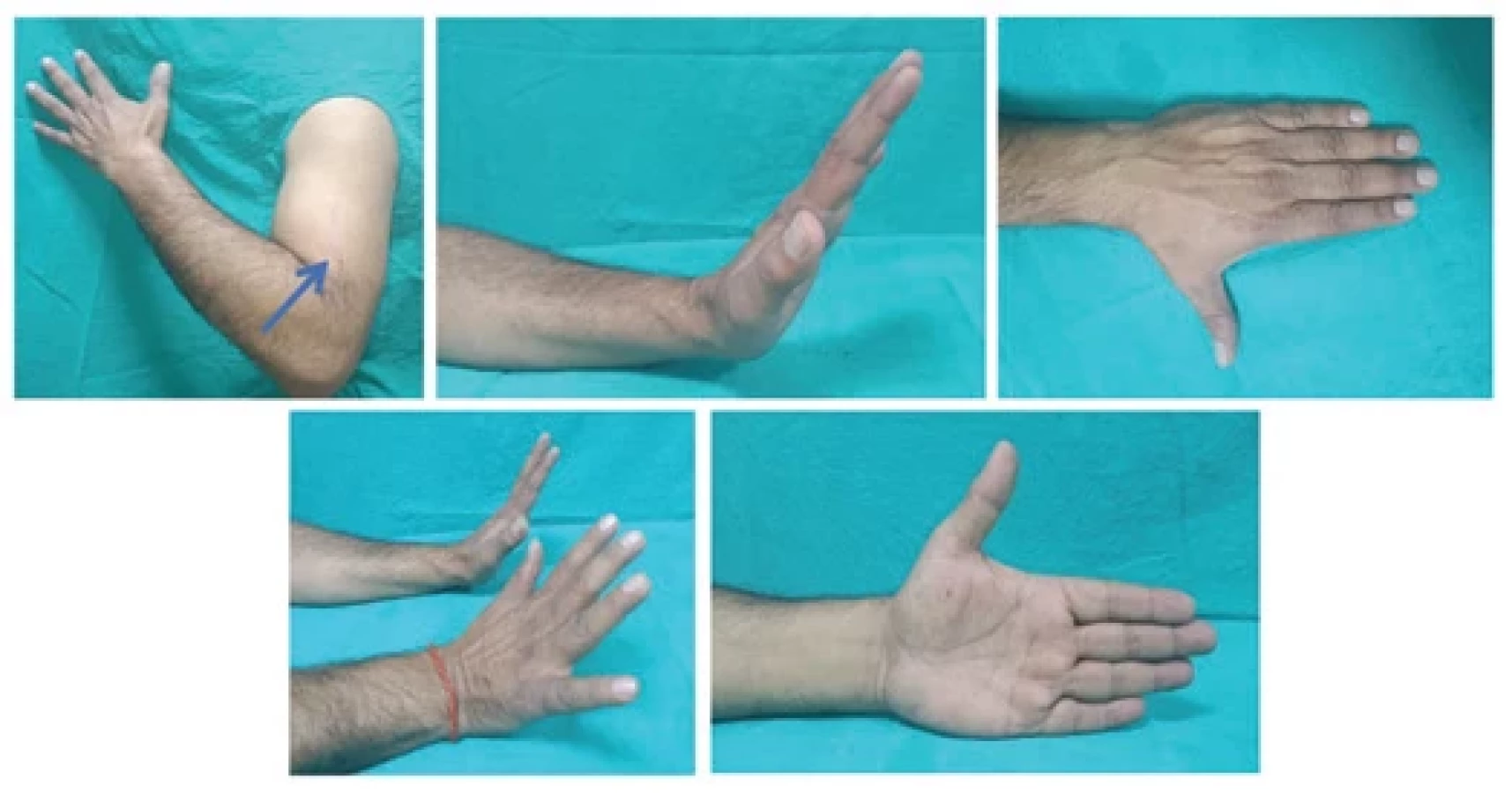
Immediate postoperatively, the patient developed a sensory deficit graded as S3+ over the radial nerve sensory distribution (BMRC scale modified by Omer and Dellon [7]), which persisted for about 8 months. However, on a one-year follow-up, sensory function had improved to S4. Motor function was fully preserved throughout, and the patient is currently asymptomatic, with complete preservation of both sensory and motor function in the radial nerve (Fig. 5).
Fig. 3. Histopathological examination (hematoxylin and eosin stain with 10× magnifi cation) showing elongated spindle-shaped cells with tapering ends, vesicular nuclei, occasional prominent nucleoli, and a moderate amount of eosinophilic cytoplasm along with Verocay body formation. Multiple areas of dilated cystic spaces and haemorrhage were noted, as well as hyalinized blood vessels and melanin pigment deposits.
Fig. 4. Immunohistochemistry of the tumor showing positivity for CD34, EMA, S100.
Fig. 5. Postoperative outcome at 6 months showing complete preservation of wrist and fi nger extension.
Case 3
A 32-year-old female manual laborer presented with a one-year-long, progressively increasing swelling in her right arm. Initially painless, the swelling became mildly painful over the last six months, worsening with heavy lifting. There were no similar swelling, and she reported no associated symptoms like numbness or weakness. She had no history of trauma, fever, appetite or weight loss, and her medical and surgical history was unremarkable.
On local examination, a 5 × 4 cm ovoid, non-tender, non-compressible, non-pulsatile, well-defined swelling was noted on the anterolateral aspect of the right mid-distal arm, approx. 15 cm proximal to the olecranon process. The borders of the swelling were distinct, and its surface was smooth. The skin over the swelling appeared hyperpigmented. The swelling was firm in consistency, mobile transversely, but had limited mobility longitudinally. Movements at the elbow and shoulder joints were normal. Tinel’s sign was negative, and no distal neurovascular deficits were noted. Axillary lymph nodes were not palpable, and routine laboratory investigations were within normal limits.
Ultrasonography suggested an intramuscular myxoma, while MRI revealed a well-defined ovoid mass in the intermuscular fat plane, likely originating from the radial nerve. A fine needle aspiration cytology study was performed, which indicated a benign spindle cell neoplasm. After discussing the prognosis and treatment options with the patient and her family, the patient was scheduled for excision biopsy.
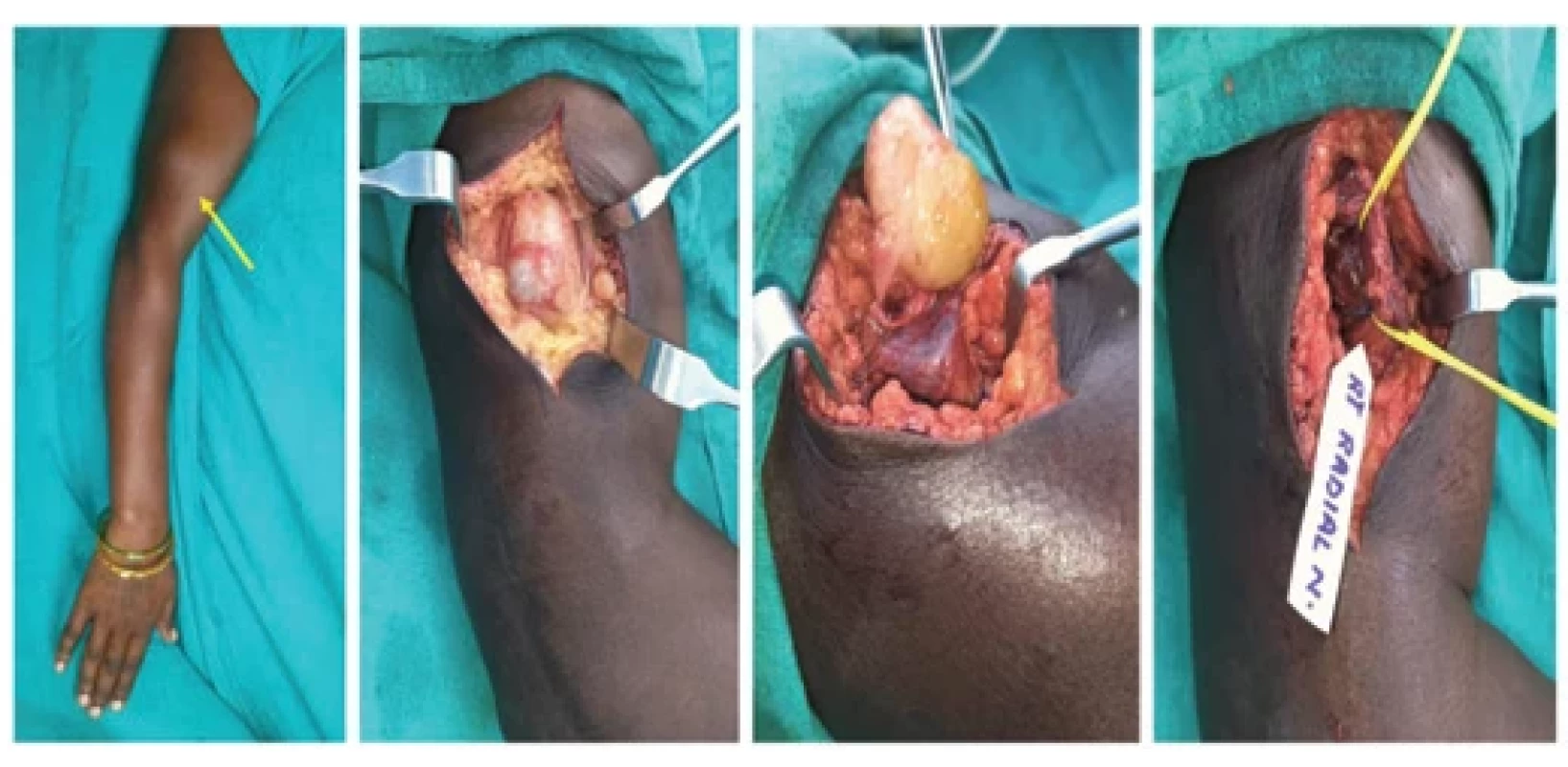
Intraoperatively, a 5 × 4 cm smooth, yellowish, ovoid mass was found in the intermuscular plane near the lateral neurovascular bundle originating from the main radial nerve before it pierced the lateral intermuscular septum, encasing the radial nerve for approx. 5 cm. Therefore, the decision was made to proceed with intracapsular enucleation of the tumor. Intraoperative assessment of radial nerve function using a nerve stimulator confirmed intact function after the tumor was removed (Fig. 6).
Histopathological evaluation confirmed the diagnosis of schwannoma, and immunohistochemistry was positive for S100 protein. On postoperative follow-up, the patient remained asymptomatic, with intact sensory and motor function of the radial nerve for up to one year post-surgery.
Fig. 6. Schwannoma arising from the right side main radial nerve. On exploration, the tumor was found to be encasing entire nerve fascicle. Hence, the tumor was completely removed by intracapsular enucleation with preservation of complete function of radial nerve.
Fig. 7. Schwannoma arising from the median nerve, the same removed with preservation of all nerve fascicles of median nerve.
Case 4
A 63-year-old male manual laborer presented with a ten-year history of progressively increasing swelling in the right forearm, which he noticed following a road traffic accident involving injury to the same area. Initially, the swelling was painless, but over the past year, he reported mild pain, tenderness, and numbness in his right hand when pressure was applied to the swelling. There were no motor deficits.
On local examination, a 12 × 10 cm minimally tender, firm, and mobile swelling was observed on the volar aspect of the proximal right forearm. The patient underwent fine needle aspiration cytology of the swelling, which confirmed the diagnosis of schwannoma.
Intraoperatively, the tumor was found to be arising from the proximal part of the median nerve. The tumor was successfully enucleated while preserving all median nerve fascicles, and histopathology confirmed the diagnosis of ancient schwannoma (Fig. 7).
Postoperatively, the patient experienced complete recovery, with no recurrence of the tumor at the one-year follow-up.
Summary of other cases
In addition to managing schwannomas arising from major motor nerves in the upper limb, we have also surgically excised schwannomas originating from sensory nerves, such as the sural nerve (Fig. 8), saphenous nerve (Fig. 9), digital nerve (Fig. 10), and lateral antebrachial cutaneous nerve (Fig. 11). Patients who presented with sensory symptoms, such as numbness and pain, experienced complete recovery from these symptoms following the surgical excision of the tumors.
Fig. 8. Schwannoma arising from left sural nerve. The tumor was arising from one of the sural nerve fascicle, which was sacrifi ced with the tumor and continuity was ensured using a vein graft harvested from the dorsum of the same foot.
Fig. 9. Schwannoma arising from the right saphenous nerve at thigh level, which was excised preserving the nerve fascicle.
Fig. 10. Schwannoma arising from multiple cutaneous nerves of the right distal leg and foot and digital nerve of the left fourth toe of the same patient. All tumors were excised with preservation of the nerve.
Fig. 11. Schwannoma rising from the left side lateral antebrachial cutaneous nerve, which was excised with preservation of the nerve fascicle.
Results and discussion
Schwannomas, also known as neurilemmomas, are common benign soft tissue tumors of the extremities, originating from the Schwann cell sheath and surrounded by a true capsule made of epineurium [2]. They account for approx. 5% of all soft tissue tumors and about 90% of all nerve tumors of ectodermal origin. Around 90% of schwannomas occur sporadically, typically in the 3rd to 6th decades of life, with no gender preference [4]. Schwannomas can be classified as proximal (arising from the brachial plexus and upper arm) or distal (arising from the forearm and hand). They may present as asymptomatic, painless swellings, or cause neurological symptoms due to nerve compression, including neurogenic pain in the extremities, local swelling, paresthesia, motor weakness, and a positive Tinel’s sign [2]. Schwannomatosis may be linked to mutations in the SMARCB1 or LZTR1 genes and can occur in both sporadic and familial forms. It primarily affects adults, with an age under 30 years serving as an exclusion criterion for the sporadic form [9].
In addition to the classical type, there are less common variants of schwannoma, including cellular, ancient, epithelioid, melanotic, and plexiform forms. Immunohistochemical analysis plays a valuable role in the differential diagnosis of peripheral nerve tumors, using monoclonal antibodies against proteins such as S-100, CD31, CD34, and GFAP [9].
Ancient schwannomas, a rare variant accounting for 0.8% of soft tissue tumors, exhibit extensive degenerative changes and nuclear atypia, often mimicking malignancy on imaging and histology [2]. Schwann cells typically stain positive for S-100 and Leu 7 markers, while epithelial membrane antigen is positive in normal, reactive, and neoplastic perineurial cells [10].
In our series, we had a total of eight patients with schwannomas, showing a male predominance of 88%. The youngest patient was 12 years old, and the eldest was 63, with a mean age of 40 years. Swelling was the most common presenting symptom, followed by pain and numbness. All patients presented with a solitary swelling, except for a 12-year-old boy who presented with multiple swellings on his foot.
The distribution of schwannomas in the body varies significantly, with these tumors most commonly found in the ear, nose, and throat regions, followed by the trunk, upper limbs (19%), and lower limbs (17.5%). Various location of schwannoma in our case series is depicted in Graph 1. While the incidence of radial nerve schwannomas is reported as 7% in literature, schwannomas arising from the main trunk of the radial nerve are relatively rare compared to those in more distal locations. However, in our case series, three patients (37.5%) presented with schwannomas originating from the main radial nerve (Graph 2).
Various benign tumors should be considered in the differential diagnosis of schwannoma, including neurofibroma, angioleiomyoma, lipoma, hemangioma, ganglion, myxoma, and xanthoma, with some rare malignant tumors [10] also in consideration. There are no distinct clinical criteria to reliably differentiate between schwannoma and neurofibroma [9].
Ultrasonography is the initial non-invasive radiological evaluation, helping to identify the location and origin of the nerve tumor and its relationship to unaffected nerve fibers. MRI is more useful in showing these tumors, typically appearing with intermediate intensity relative to muscles on T1-weighted images and hyperintense on T2-weighted images. Schwannomas usually exhibit uniform enhancement, although larger tumors may show more heterogeneous enhancement. A post-contrast T1-weighted sequence can help distinguish the tumor from the surrounding nerve fascicles.
Radiological differentiation of schwannomas from other tumors can be challenging, as most imaging studies reveal similar hypoechoic masses with distal sound enhancement. Although MRI is more accurate in diagnosing schwannomas, it is not 100% reliable. Electrodiagnostic tests, like electromyography, may yield normal results in the absence of neurological deficits, since only a small portion of the nerve fibers is typically affected. Needle or open biopsy is not routinely recommended, as it can cause scarring and fascicular damage [11].
Malignant peripheral nerve sheath tumors pose a significant challenge for specialists, typically occurring in the trunk and extremities, with rare cases in other locations. About half are linked to neurofibromatosis type 1 (NF1), while others arise spontaneously (40%) or after radiation therapy (10%). MRI is the preferred diagnostic tool, but FDG-PET shows promise in distinguishing benign from malignant NF1-associated tumors, potentially reducing the need for biopsy. Wide local excision is the primary treatment, with limb amputation considered in non-metastatic cases. Recurrence rates can reach 65%, with a five-year survival ranging from 16% to 52% [12]
In cases of neurological deficits following tumor resection, neurorrhaphy or nerve grafting may be considered [3]. Improvement in nerve function is typically achieved, and the onset of new, persistent postoperative deficits is rare. The slow growth of schwannomas allows nerve function to adapt to the pressure effects, but once the tumors become symptomatic, surgical excision remains the definitive treatment [13].
The evaluation of postoperative outcomes showed that one patient experienced mild motor weakness immediately following surgery, with no cases of permanent motor deficits reported. Four patients exhibited sensory deficits in the early postoperative period, while one patient had a sensory deficit that persisted for approx. eight months but fully resolved by the one-year follow-up. Notably, there were no incidences of postoperative complications such as seroma, hematoma, wound infection, or symptom recurrence during the entire one-year follow-up period (Tab. 3).
Surgical removal of the peripheral nerve schwannoma is generally a safe procedure, offering favourable functional outcomes with a minimal risk of post operative motor and sensory defecits [14].Surgery with the aid of intraoperative nerve monitoring can reduce the risk of complications and help presrve neurological function, particularly when there is no preexisting functional impairement. For patients with peripheral nerve schwannomas who are asymptomatic, a watchful waiting approach may be suitable given the benign nature of these tumors. However, symptomatic tumors requires carefull planning and excision.
Graph 1. The distribution of the various locations in the body aff ected with schwannoma.
Graph 2. The distribution of aff ected nerves.
Tab. 3. Complete postoperative functional outcome of all patients.
Conclusion
Peripheral Schwannomasoriginating from nerves such as the radial and median erves are rare but should be considered in the differential diagnosis of the soft tissue tumors of the extremities.MRI serves as an essential imaging tool for preoperative diagnosis while histopathological evaluation and immunohistochemistry confirms the diagnosis and rules outother common differentials. Surgical enucleation or intracapsular excision remains the primary treatment option.
writing: original draft preparation – Jiten Kumar Mishra, Shamendra Anand Sahu, Abhijith Valsalan; writing: review and editing – Jiten Kumar Mishra, Shamendra Anand Sahu, Abhijith Valsalan, Moumita De.
Disclosure
The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Zdroje
1. Ansilata Marlyn AM., Ameer F., Pal HK. Case report of schwannomas: benign tumour of the peripheral nerve sheath. EMJ Neurology. 2020, 8 (1): 103–107.
2. Hakan T., Kılıç Y., Çelikoğlu E., et al. An unusual schwannoma in the proximal forearm: a case report. Cureus. 2019, 11 (11): e6231.
3. Kang HS., Teong CT., Park JE., et al. Incomplete high radial nerve palsy due to schwannoma of radial nerve in the upper arm – a case report. Open J Orthop. 2017, 7 (2): 72–78.
4. Felimban M. The first reported case of schwannoma of superficial radial nerve in the forearm in Saudi Arabia. Surg Curr Res. 2022, 12 (8): 1–3.
5. Silva GB., Lima MR., Cho AB., et al. Gracilis muscle transfer to elbow flexion in brachial plexus injuries. Acta Ortop Bras. 2020, 28 (4): 165–167.
6. Paprottka FJ., Wolf P., Harder Y., et al. Sensory recovery outcome after digital nerve repair in relation to different reconstructive techniques: meta-analysis and systematic review. Plast Surg Int. 2013, 2013 : 704589.
7. Dellon AL. The moving two-point discrimination test: clinical evaluation of the quickly adapting fiber/receptor system. J Hand Surg. 1978, 3 (5): 474–481.
8. Omer GE. Methods of assessment of injury and recovery of peripheral nerves. Surg Clin North Am. 1981, 61 (2): 303–319.
9. Senol N., Yilmaz O. A rare type of peripheral nerve sheath tumor: radial nerve schwannoma. Turk Neurosurg. 2015, 25 (1): 137–140.
10. Perentes E., Nakagawa Y., Ross GW., et al. Expression of epithelial membrane antigen in perineurial cells and their derivatives. Acta Neuropathol. 1987, 75 (2): 160–165.
11. El Sayed L., Masmejean EH., Lavollé A., et al. Clinical results after surgical resection of benign solitary schwannomas: a review of 150 cases. Orthop Traumatol Surg Res. 2022, 108 (4): 103281.
12. Guha D., Davidson B., Nadi M., et al. Management of peripheral nerve sheath tumors: 17 years of experience at Toronto Western Hospital. J Neurosurg. 2018, 128 (4): 1226–1234.
13. Gosk J., Gutkowska O., Urban M., et al. Results of surgical treatment of schwannomas arising from extremities. Biomed Res Int. 2015, 2015 : 547926.
14. Zipfel J., Al-Hariri M., Gugel I., et al. Surgical management of sporadic peripheral nerve schwannomas in adults: indications and outcome in a single center cohort. Cancers. 2021, 13 (5): 1017.
15. Kampel L., Serafimova M., Edalati S., et al. Functional outcome following intracapsular resection of head and neck peripheral nerve sheath tumors: a retrospective cohort. J Otolaryngol Head Neck Surg. 2023, 52 (1): 65.