
Laparoscopic resection of retroperitoneal metastasis originating from sternal leiomyosarcoma – a case report
Laparoskopická resekce retroperitoneální metastázy pocházející ze sternálního leiomyosarkomu – kazuistika
Východiska: Leiomyosarkomy jsou malignity hladkého svalstva, které mohou časně metastazovat hematogenním šířením. Leiomyosarkom sterna je extrémně vzácný, mezi maligními nádory kostí má incidenci < 0,7 %. Případ: Prezentujeme případ 66letého muže s retroperitoneální metastázou lokalizovanou v pravém pararenálním prostoru, pocházející z leiomyosarkomu sterna. Pacient před 3 lety podstoupil parciální resekci sterna a žeberních chrupavek následnou osteosyntézou hrudní stěny kvůli primárnímu nádoru. V rámci dalšího sledování CT a PET-CT odhalily masu v pravém perirenálním prostoru, mezi horním pólem pravé ledviny a pravou nadledvinou. Při absenci dalších metastatických lézí a po rozhodnutí multidisciplinárního onkologického týmu byla provedena laparoskopická en bloc metastazektomie a pravostranná adrenalektomie. Výsledky: Histopatologické vyšetření potvrdilo metastatickou povahu nádoru s negativními resekčními okraji. Pooperačně se u pacienta objevila horečka způsobená atelektázou, která byla zvládnuta intravenózními antibiotiky. Z nemocnice byl propuštěn šestý pooperační den a po dvouletém sledování je bez recidivy. Závěr: Minimálně invazivní chirurgické techniky umožňují onkologickou resekci retroperitoneálních metastatických lézí s nízkou perioperační morbiditou a mortalitou. Bylo prokázáno, že resekce izolovaných metastáz do lymfatických uzlin zlepšuje celkové přežití a kontrolu onemocnění.
Klíčová slova:
Adrenalektomie – leiomyosarkom – Sternum – retroperitoneální metastáza – metastáza do lymfatických uzlin – minimálně invazivní metastazektomie
Authors:
O. Ioannidis 1; E. Kotidis 1; E. Anestiadou 1; I. Matzarakis 2; J. P. Skliris 2; S. Symeonidis 1; S. Bitsianis 1; O. Kerasidou 1; M. Kaprianou 1; C. Chatzianestiadou 1; E. Salta-Poupnara 1; F. Tserkezidis 1; K. Angelopolos 1; S. Angelopoulos 1
Authors place of work:
Fourth Department of Surgery, Medical School, Faculty of Health Sciences, Aristotle University of Thessaloniki, General Hospital, “George Papanikolaou”, Thessaloniki, Greece
1; Department of Pathology, General Hospital “George Papanikolaou”, Thessaloniki, Greece
2
Published in the journal:
Klin Onkol 2025; 38(4): 302-306
Category:
Kazuistiky
doi:
https://doi.org/10.48095/ccko2025302
Summary
Background: Leiomyosarcomas are malignancies of smooth muscle differentiation that can metastasize early through hematogenous spread. Leiomyosarcoma of the sternum is extremely rare, with an incidence of < 0.7% among malignant bone tumors. Case: We report the case of a 66-year-old male with a retroperitoneal metastasis located in the right pararenal space, originating from a sternal leiomyosarcoma. Three years earlier, the patient had undergone partial excision of the sternum and costal cartilages, followed by thoracic wall osteosynthesis, for the primary tumor. Follow-up imaging with CT and PET-CT revealed a mass in the right perirenal space, situated between the upper pole of the right kidney and the right adrenal gland. In the absence of other metastatic lesions and following multidisciplinary oncology team discussion, the patient underwent laparoscopic en bloc metastasectomy and right adrenalectomy. Results: Histopathological examination confirmed the metastatic nature of the tumor with negative resection margins. Postoperatively, the patient experienced fever due to atelectasis, which resolved with intravenous antibiotics. He was discharged on the 6th postoperative day and remains free of recurrence at a two-year follow-up. Conclusion: Minimally invasive surgical techniques allow for oncological resection of retroperitoneal metastatic lesions with low perioperative morbidity and mortality. Resection of isolated lymph node metastases has been shown to improve overall survival and disease control.
Keywords:
Adrenalectomy – Sternum – Leiomyosarcoma – lymph node metastasis – retroperitoneal metastasis – minimally invasive metastasectomy
Introduction
Primary leiomyosarcoma (LMS) of the bone was first described in 1965 by Evans and Sanerkin and is a rare and aggressive primary osseous sarcoma, representing less than < 0.7% of all primary malignant bone tumors [1,2]. It is a high--grade destructive osseous tumor with poor prognosis, depending on the stage at diagnosis, and may arise de novo or after previous radiation [3,4]. Primary leiomyosarcoma of the sternum is an extremely uncommon clinical entity, with few references reported in the literature worldwide [5,6]. Surgical resection is highly due to a poor prognosis of 35% overall survival (OS) rate [6]. The following case report is about a 66-year old patient, presented with retroperitoneal metastasis secondary to primary leiomyosarcoma of the sternum excised two years before, and is described in accordance to the Case Report (CARE) guidelines [7]. Both the patient and his relatives were thoroughly informed and a written informed consent was obtained for publication of the present case report and the accompanying images. Copies of the written consent are available for review by the Editor-in--Chief of this journal. The present study highlights the importance of awareness of primary bone leiomyosarcoma metastatic potential, as well as the role of minimally invasive surgery in achieving low morbidity and mortality rates after resection of isolated metastatic lesions.
Case report
We report a case of a 66-year-old male, diagnosed with primary leiomyosarcoma of the sternum three years before, without history of irradiation. Past medical history was free of comorbidities. Partial sternal resection along with resection of adjacent chest wall structures with negative fatty margins and reconstruction of thoracic wall with methylmethacrylate prosthesis was performed. No adjuvant therapy followed, after making shared decisions with the patient due to confirmation of negative margins in the final pathology report. The postoperative course was uneventful and without any symptoms, until a nodal metastatic lesion in the retroperitoneum was encountered at a three--year follow-up. Particularly, follow-up computed tomography revealed a solitary metastatic lesion in the right pararenal space, between the upper pole of the right kidney and the right adrenal gland, measuring 4.1 × 3.3 × 3.5 cm (Fig. 1). The lesion was in close proximity to the right renal vein and seemed to be infiltrating the right adrenal gland. PET-CT also confirmed the aforementioned finding, revealing a hypermetabolic lesion in the right pararenal space, with no signs of recurrence in the chest wall. The rest of laboratory data, including serum levels of alkaline phosphatase, calcium, phosphate, and tumor markers, were normal. Core needle biopsy was also performed and the histopathological examination was indicative of a metastatic mesenchymal malignant neoplasm compatible with leiomyosarcoma. Based on long disease-free interval, absence of other metastatic lesions and good physical and biological status of the patient, the oncology group approved the surgical management. The patient underwent en block laparoscopic surgical excision of the retroperitoneal metastatic lesion, combined with right adrenalectomy due to the assumed infiltration of part of the adrenal gland. Under general anesthesia, the patient was placed in a full lateral left decubitus position. Transperitoneal approach for was chosen and four ports were used. Severe adhesions were noted around the right adrenal central vein. This area was dissected by sharp dissection and the metastatic nodal mash was completely resected macroscopically en block with the right adrenal gland. The operative time was 135 minutes, and blood loss was minimal. Immediately after surgery, the patient returned to the ward and remained stable. On the 2nd postoperative day, he developed fever up to 38.3 °C, which was attributed to atelectasis, based on chest X-rays and after pulmonary consultation, intravenous antibiotic coverage with piperacillin/tazobactam and intensive respiratory physiotherapy began. The patient was discharged on 7th postoperative day.
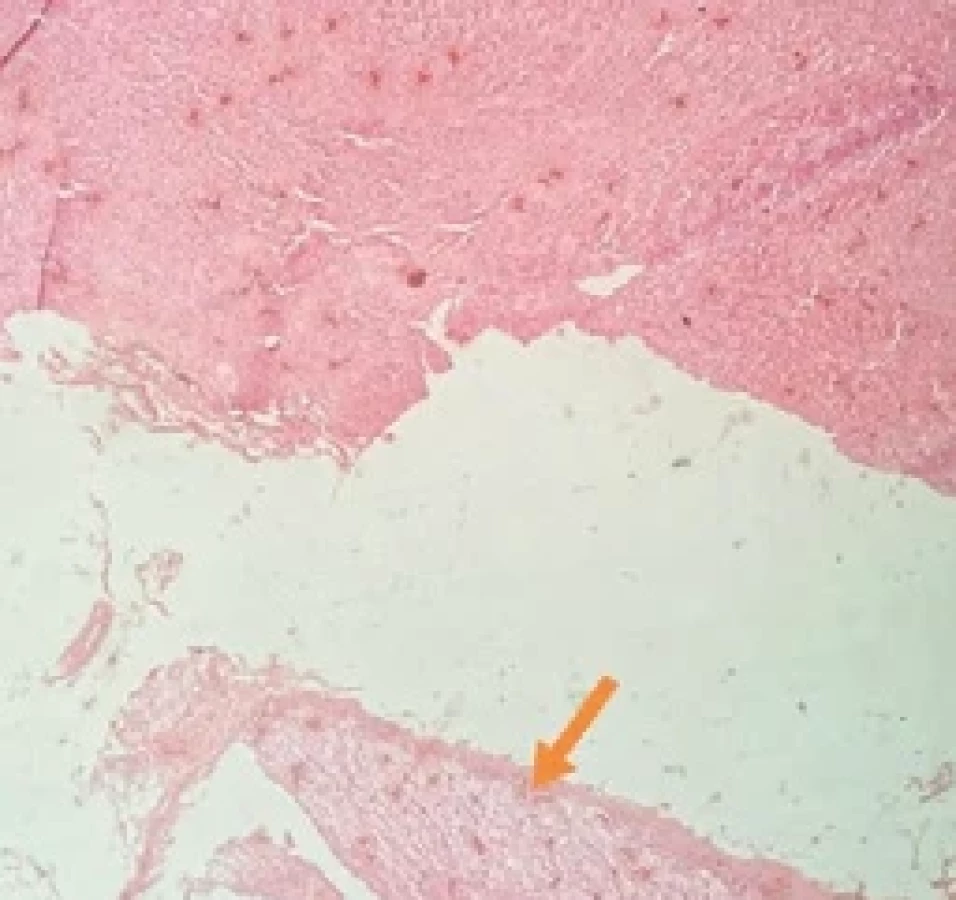
The mass was sent for histological examination. The mass was solid and whitish and measured 5.7 × 4.5 × 4 cm. The histology report confirmed the preoperative diagnosis of retroperitoneal metastasis originating from the primary sternal leiomyosarcoma, as well as the negative resection margins (Fig. 2), describing a mesenchymal malignant tumor with neoplastic cells exhibiting marked pleomorphism and increased mitotic activity (Fig. 3). During immunohistochemical evaluation, tumor cells stained positive for caldesmon and desmin (Fig. 4, 5). No adjuvant therapy was administered. At a two-year follow-up, the patient remains free of symptoms and recurrence, according to the findings of physical examination, whole body CT, and PET-CT.




Discussion
Primary LMS of the bones represents an uncommon malignant intraosseous neoplasm, characterized by spindle cells with smooth muscle differentiation, without matrix production [8]. It represents less than 0.7% of all malignant bone tumors and, thus, knowledge of biology and clinical behavior is limited [9]. Main locations affected include the long bones, particularly distal femur and proximal tibia, in 70% of cases, followed by the craniofacial bones in about 20% of the cases [4]. Sternum primary leiomyosarcoma is extremely rarely reported in the literature. Aoki et al. described a case of primary postirradiation LMS of the sternum in a patient who had received irradiation due to mediastinal seminoma 11 years ago. The management plan included preoperative chemotherapy with cisplatin, doxorubicin and IFOVADEC (ifomide, vindesine, doxorubicin, and dacarbazine), as well as resection of the upper one-third of the sternum, the medial one-third of the bilateral clavicles, and the anterior part of the first, second, and third ribs. The authors mention that the patient remained recurrence-free during a three-year follow-up [5]. A case of chest wall leiomyosarcoma affecting the left 7th, 8th, and 9th ribs was also described by Nagai and colleagues, which was managed with chest wall resection and reconstruction with polypropylene mesh. The patient underwent a total of three liver metastasectomies, three lung metastasectomies, and proton-beam radiotherapy for sacral metastasis, and was still of recurrence 14 years after chest surgery [10].
Leiomyosarcomas, however, are more common in uterus, gastrointestinal tract, and retroperitoneum, presenting as abdominal masses [11]. Particularly, the retroperitoneum is a common site of origin of leiomyosarcomas, constituting 12–69% of cases [12]. Therefore, clinical examination and a thorough investigation are important to distinguish a primary tumor from a metastatic one [5]. In our case, this was achieved by core needle biopsy.
Primary bone leiomyosarcoma should be managed by multidisciplinary teams in specialized reference centers [2]. Surgical excision with negative margins remains the cornerstone of management [2]. Adjuvant therapy with chemoradiation is recommended in case of positive specimen margins [6]. However, leiomyosarcoma of the bone is accompanied by metastasis in 50% of patients within 33 months, especially in those patients treated by surgical resection only, as in the case presented [5].
Few data are available regarding optimal management of metastatic leiomyosarcoma of the bone [5]. A case series by Rekhi et al. showed that metastatic potential in these tumors is high, independent of tumor stage [13]. In addition, metastatic disease is more likely to present within the first year after the appearance of the primary tumor, with the lungs being the most common site of metastasis, while metastases to the liver, adrenal glands, kidneys, and lymph nodes have also been reported, but with a lower rate [2]. Chemotherapy is often used in combination with personalized management and is also the main option for palliative treatment [5]. Recine et al. highlight the poor outcome of surgical resection of metastatic leiomyosarcoma of the bone, while some other authors propose that complete surgical resection of the tumor offers longer overall survival rates [2]. According to Katsuhiro et al., metastasectomy for patients with advanced soft tissue sarcomas should be performed only if potential advantages outweigh disadvantages [14]. Palliative cryoablation has also been proposed for advanced unresectable malignancies causing compression effects [15]. So, no commonly accepted guidelines have been established about the management of metastatic leiomyosarcoma of the bone due to poor prognosis and limited cases reported.
Conclusion
Primary leiomyosarcoma of the bone is a scarce but aggressive clinical entity, with few reports of cases originating from the sternum. More clinical trials are necessary in order to improve the knowledge of the disease’s biology and metastatic potential, as well as to enrich our armamentarium with targeted therapeutic agents. There is no consensus and established guidelines regarding the role of surgery and adjuvant therapy in metastatic disease. However, minimally invasive surgery seems to offer the opportunity for excision of retroperitoneal metastatic lesion with minimal morbidity and mortality rates.
Statements
All authors undersigned certify that they do not have any financial or personal relationships that might bias the content of this work.
All authors undersigned certify that they have the written consent of the identifiable person in order to present the case in this scientific paper.
Zdroje
1. Evans DM, Sanerkin NG. Primary leiomyosarcoma of bone. J Pathol Bacteriol 1965; 90 (1): 348–350. doi: 10.1002/path.1700900145.
2. Recine F, Bongiovanni A, Casadei R et al. Primary leiomyosarcoma of the bone: a case report and a review of the literature. Medicine 2017; 96 (45): e8545. doi: 10.1097/MD.0000000000008545.
3. Brewer P, Sumathi V, Grimer RJ et al. Primary leiomyosarcoma of bone: analysis of prognosis. Sarcoma 2012; 2012 : 636849. doi: 10.1155/2012/636849.
4. Wang GY, Lucas DR. Primary leiomyosarcoma of bone review and update. Arch Pathol Lab Med 2019; 143 (11): 1331–1337. doi: 10.5858/arpa.2019-0375-RA.
5. Aoki T, Ozeki Y, Watanabe M et al. Development of primary leiomyosarcoma of the sternum postirradiation: report of a case. Surg Today 1998; 28 (12): 1326–1328. doi: 10.1007/BF02482828.
6. Rossi M, DiSilvio F, Sahagun J et al. Primary sternal leiomyosarcoma. Ann Thorac Surg Short Rep 2024; 3 (1): 219–221. doi: 10.1016/j.atssr.2024.07.006.
7. Gagnier JJ, Kienle G, Altman DG et al. The CARE guidelines: consensus-based clinical case reporting guideline development. J Med Case Rep 2013; 7 : 223. doi: 10.1186/1752-1947-7-223.
8. Schajowicz F. Tumors and tumorlike lesions of bone: pathology, radiology and treatment. 2nd ed. Springer-Naute 2012.
9. Jin X, Chen AL, Liu W. Case report a rare case report of primary leiomyosarcoma of distal femur bone in a patient with multiple myeloma and review of literature. N Am J Med Sci 2020; 14 (1): 24–27. doi: 10.7156/najms.2020.1301024.
10. Nagai S, Imanishi N, Miura K et al. The case of a long-term survivor of chest wall leiomyosarcoma who underwent chest wall resection followed by repeated metastatectomies. J Japan Assoc Chest Surg 2017; 31 (6): 747–752.
11. Cho DH, Lee JH, Oh BC. Unusual presentation of retroperitoneal leiomyosarcoma mimicking an adnexal tumor with highly elevated serum CA-19-9. Obstet Gynecol Sci 2014; 57 (1): 77–81. doi: 10.5468/ogs.2014.57.1.77.
12. Marko J, Wolfman DJ. Retroperitoneal leiomyosarcoma. Radiographics 2018; 38 (5): 1403–1420. doi: 10.1148/rg.2018180006.
13. Rekhi B, Kaur A, Puri A et al. Primary leiomyosarcoma of bone – a clinicopathologic study of 8 uncommon cases with immunohistochemical analysis and clinical outcomes. Ann Diagn Pathol 2011; 15 (3): 147–156. doi: 10.1016/j.anndiagpath.2010.11.006.
14. Hayashi K, Hiraoka K, Akiyama T et al. Benefit of surgical resection of distant metastasis in soft tissue sarcoma: a systematic review. Jpn J Clin Oncol 2021; 51 (7): 1088–1093. doi: 10.1093/jjco/hyab049.
15. Dimopoulos MP, Giannikas N, Kitrou PM et al. Palliative cryoablation of leiomyosarcoma of the sternum compressing the heart. J Vasc Interv Radiol 2024; 35 (6): 944–945. doi: 10.1016/j.jvir.2024.01.021.
Štítky
Detská onkológia Chirurgia všeobecná OnkológiaČlánok vyšiel v časopise
Klinická onkologie

2025 Číslo 4
- Brno opět přivítá onkology a nelékařské zdravotnické pracovníky
- I „pouhé“ doporučení znamená velkou pomoc. Nasměrujte své pacienty pod křídla Dobrých andělů
- Realita liečby bolesti v paliatívnej starostlivosti v Nemecku
- MUDr. Lenka Klimešová: Multiodborová vizita je kľúč k efektívnejšej perioperačnej liečbe chronickej bolesti
- Fixní kombinace tramadol/paracetamol je doporučenou volbou v léčbě chronické bolesti v ordinaci praktického lékaře
Najčítanejšie v tomto čísle
- Popis TEMPI syndromu při Waldenströmově makroglobulinemii
- Od tradiční čínské medicíny po molekulární onkologii – pleiotropní účinky tauroursodeoxycholové kyseliny
- Integrativní medicína v onkologii – mezi vědou, ideologií a pragmatizmem
- Vliv a stanovení lidského cytomegaloviru u onkologických onemocnění