
Comparing the epidemiological situation of selected sexually transmitted infection in three Czech regions between 2006 and 2013
Porovnání vývoje epidemiologické situace vybraných sexuálně přenosných infekcí ve třech krajích České republiky v letech 2006–2013
Cíl: Studie se zaměřuje na identifikaci hlavních rozdílů ve výskytu vybraných sexuálně přenosných infekcí v třech krajích České republiky.
Metody: Deskriptivní průřezová studie analyzuje data získaná z jednotlivých institucí disponujících přístupy do Registru pohlavních nemocí za jednotlivé kraje. Do studie vstupovaly celkem tři kraje, přičemž do studie byla integrována pouze ta data, která se vyskytují v časově stejném intervalu ve všech krajích (tj. v letech 2006–2013). Pro porovnání vývoje epidemiologické situace byla použita míra incidence (incidence rate – IR) a specifická míra incidence výskytu (specific incidence rate –SIR) pro věk a věkové skupiny. Byly implementovány metody deskriptivní statistiky. Pro analýzu statisticky významných rozdílů byla použita ANOVA při p = 0,01, případně nepárový T-test, kterému předcházel F-test pro testování rozptylů.
Výsledky: Nejvyšší incidence rate pro všechny integrované STIs byla uváděna v kraji Hlavní město Praha (HMP) 398,3 případů na 100 tisíc obyvatel, přičemž nejčastěji se vyskytovala ve dvou krajích kapavka (HMP) a Středočeský kraj (STR), zatímco v Plzeňském kraji (PLZ) se nejčastěji vyskytovala syfilis. ANOVA identifikovala statisticky významné rozdíly mezi všemi integrovanými kraji v rámci výskytu všech STIs jako skupiny infekcí i jednotlivých STIs. Ovšem T-test identifikoval statisticky signifikantní rozdíly ve většině případů pouze mezi HMP a zbylými dvěma kraji, avšak mezi PLZ a STR tyto rozdíly identifikovány nebyly. Rovněž byly identifikovány statisticky významné rozdíly (ANOVA pro všechny tři kraje vzájemně) pro SIR pohlaví a věkovou skupinu 15–64 let, kde bylo agregováno nejvíce případů. Ve všech krajích bylo více mužů (HMP 75 %, PLZ 58,7 % a STR 66 %). Většinu případů tvořili Češi (69,7–79,8 %). Koinfekce HIV byla reportována u HMP v 5,5 % případů u PLZ 3,9 % a u STR 5,3 %.
Závěr: Studie předkládá výsledky porovnání dat ze tří krajů Česka za období 2006–2013. Poukazuje na rozdíly ve vývoji sexuálně přenosných infekcí v jednotlivých krajích a v některých atributech, zejména u mužů majících sex s muži a dalšími rizikovými skupinami. Apeluje rovněž na nedostatečnou znalost problematiky sexuálně přenosných infekcí u subpopulace MSM.
Klíčová slova:
Česká republika – sexuálně přenosné infekce – ANOVA – T-test – sexuální zdraví
Authors:
J. C. Sekera
Authors place of work:
Přírodovědecká fakulta Univerzity Karlovy, Praha
Published in the journal:
Epidemiol. Mikrobiol. Imunol. 71, 2022, č. 4, s. 190-202
Category:
Původní práce
Summary
Aim: The research aimed to identify and describe the main differences in the incidence of sexually transmitted infections in three regions of the Czech Republic.
Methods: Descriptive cross-section study analyses data received from each institution that allowed access to the Registry of sexually transmitted illnesses of individual regions. Mainly three regions are being studied, yet the study considers only the data from the same time-period in all three regions (i. e., 2006–2013). To compare the development of the epidemiological situation, we considered the incidence rate (IR) and specific incidence rate for both age and age groups. Methods of descriptive statistics were implemented. For the analysis of statistically significant differences, we used ANOVA when p = 0.01, alternatively in some cases F-test before an unpaired T-test to test variability.
Results: The highest incidence rate for all integrated STIs was reported in the Capital City of Prague region (CCP) – 398.3 cases per 100 thousand – whereas gonorrhoea appeared the most in CCP and Central Bohemia regions (CBR) and syphilis occurred the most in the Pilsen region (PLS). ANOVA identified statistically significant differences between all integrated regions within the frame of incidence of all STIs as a group of infections, and also as individual STIs. Of course, the T-test identified statistical differences in most cases only between CCP and the other two regions, even though these differences weren’t identified between CBR and PLR. Likewise, there were statistically important differences identified (by ANOVA for all three regions mutually) for the specific incidence rate for gender and the 15–64 age group category where the most cases were aggregated. In all three regions, there were more male cases (CCP 75%, PLR 58,7% and CBR 66%) with most of them being composed of Czechs (69.7–79.8 %). HIV coinfection was reported in 5.5% of cases in CCP, 3.9% in PLR and 5.3% in CBR.
Conclusion: This study submits the results of data comparison from three Czech regions in the 2006–2013 time-period. It points out differences in the development of sexually transmitted infections in individual regions, mainly in men having sex with men and other risk groups. It also invokes the issue of the insufficient level of knowledge concerning sexually transmitted infections in the MSM subpopulation.
Keywords:
sexually transmitted infections – Czech Republic – ANOVA – T-test – sexual health
INTRODUCTION
Sexually transmitted infections (STIs) present a long - -term and global problem. This group of infections, mostly transmitted sexually, is the main problem faced by public healthcare [1]. The occurrence of this rather specific group of infections is primarily determined by health status, education, poverty, and unemployment [2]. Despite that most of these infections have effective treatment (with exception of HIV, the chronic HSV infection and others), they carry complications in the forms of pelvic inflammatory disease, epididymitis, infertility, cervical cancer, cardiovascular and neurological damage, mortality, and also increasing resistance to antibiotics [1].
According to the reports of the European Centre for Disease Prevention (ECDC), the incidence of syphilis is on the rise since 2010, especially in men whereas in the year 2017, the incidence of this illness in the European Union (EU) was 7.1 cases per 100 thousand [3]. The surge of syphilis towards the end of the 20st century was preceded by the reduction of its occurrence due to fears of the HIV infection [1], which arose due to changes in sexual behaviour and social norms, drug usage, increasing migration, travel development, and as well as result of insufficient investments into public healthcare services [4]. Among other things, this study [4] points at the fact that syphilis appears in three “categories”: population majority in developing countries, in minority populations with low socio-economic status in developed countries and men having sex with men (MSM). In the 2013–2016 period, syphilis was associated with 300 thousand foetal and neonatal deaths and 215 thousand new-borns, who are exposed to the risk of earlier death as result of this illness [5]. In the Czech Republic, the highest incidence level of syphilis was reached in the year 2010 (9.7 cases per 100 thousand). The epidemy is moving towards higher age categories and it is manifested more in the foreigner ratio, for example in the year 2006 (31.9%) [6].
In contrast to syphilis, the occurrence level of gonorrhoea is much higher; in the EU countries, it consisted of 26.4 cases per 100 thousand (2018), which is a 22% increase to the previous year. From this number, 48% was formed by MSM [7]. The epidemy is evidently of much wider nature, as even though MSM forms 48% of new cases. Men form a group of individuals for whom gonorrhoea is mostly symptomatic, while in women this value is around 50% [1]. In the Czech Republic, gonorrhoea is reported more often in lower age categories [8] than syphilis. Same as with syphilis and much like in many other European countries, the gonorrhoea epidemy in the Czech Republic has constantly decreased since the 1970s. The end of this constant decrease was reported until the 1990s and at the beginning of the new millennium the gonorrhoea epidemy began growing [9]. The highest prevalence of gonorrhoea in the Czech Republic was reported in 2007 when it reached the value of 11.1 cases per 100 thousand; similar numbers were reached also in the year 2012 [8].
Whereas in East and West Africa, India, South-East Asia and the Caribbean the genital infection lymphogranuloma venereum (LGV) forms 1–10%, in developed countries the incidence is very low [10]. However, its incidence is on the rise since 2003 when from a formerly tropical illness with very sporadic and imported occurrence in developed countries it became endemically spread in the MSM subpopulation in developed countries [11]. Its import into Europe, followed by its spread in North America through the spread among MSM, is connected to Rotterdam where a case appeared which was then associated with its spread to many other countries [12]. In the EU, the occurrence of LGV is often associated with HIV as its coinfection as well as with other infections such as HCV (19%) and other STIs (39%) [1]. The epidemiological situation in the Czech Republic is very similar to that in the EU where most cases are male (99%), the MSM ratio is also devastating [13] and the long-term prevalence is around 0,1 cases per 100 thousand [8].
The following infections fall under compulsory reporting in the Czech Republic: early syphilis, congenital syphilis, late syphilis, other and unspecific syphilis, gonococcal infection, lymphogranuloma venereum and chancroid. These infections are coded according to MKN-10 (A50–A55 and A57). The collection of this data stems from act no. 258/2000 Sb. regarding the protection of public health, act no. 306/2012 Sb. regarding conditions to avoid the occurrence and spread of infectious illnesses and hygienic demands to the running of healthcare facilities and social care institutions and also act no. 473/2008 Sb. concerning the system of epidemiological alertness of selected infections in the amendment of later [6].
Mandatory reporting is aggregated in the Register of Venereal Diseases (RVD) that falls under the Institute of Health Information and Statistics of the Czech Republic [6]. Specific cases (defined in the RVD as statistic units) are inserted by Regional Public Health Authorities that transcribe information sent in by doctors who identified the infections [6].
This study presents the first study focussed on sexually transmitted infections working with individual data from three regions in the Czech Republic. From its conclusions more specific questions can arise concerning deeper epidemiological analysis, alternatively for more effective of primary prevention for the subpopulations at risk. The study’s goal is to find out whether the three selected regions statistically differ from each other, and also what are their similarities.
METHODS
Descriptive cross-section study analyses the primary data extracted from screening reports from the delimited period 2006-2013. The data was provided from three regions in the Czech Republic: Capital City of Prague, Pilsen and Central Bohemia.
Each region manages access of other institutions to the Register of Venereal Diseases (RVD). It is provided by regional public health offices in the Capital City of Prague and Central Bohemian regions, alternatively by regional archives if the shredding period has elapsed. In the last region (Pilsen), it is the Department of Dermato - venereology that disposes access to data of the University Hospital of Pilsen. Considering the time-consuming process of extracting data through simple transcription of the screening paper reports (necessary to gain individual data), there are different accessibility intervals. The selected period 2006-2013 represents the intersection of accessibility years in all integrated regions. It was necessary to certify discretion and to confirm anonymous processing of the data. Most variables are of nominable, alternatively ordinal character (e.g., education), which partially limits analysis. The reporting of venereal diseases is included in the document containing basic information about the patient. In the course of the tracked period, a new form was created and applied, therefore some variables were eliminated from the analysis. Only the data that were present in all data files were analysed (one data file per region). Individual data presented information about the patient’s year of birth (at the time of the diagnosis), gender, district and region of residence, ethnicity, the equipment that diagnosed them, the department that diagnosed (specialisation), education, economic activity, family status, mode of transmission (heterosexual, homosexual), sexual risks, occurrence of illness, when the illness was detected, pregnancy, HIV status, medications, number of reference contacts and the source.
Data present information about the newly diagnosed cases, therefore the incidence rate was calculated for individual infections (syphilis, gonorrhoea, LGV) and then for all STIs collectively within the frame of individual years or defined interval (middle class population as denominator of the given interval). We then worked with a specific incidence rate for age and gender. The data to calculate incidence rate was obtained from the Czech Statistical Office [20], mainly concerning the population in individual districts and regions and then the age and gender groups in each of them.
The data was processed in the programmes SPSS, MS Excel and also ArcGIS online to create map outputs. Descriptive statistics bring information about the frequency of examined variables in each individual region in absolute and also relative value. Besides these variables, the descriptive statistics analysed average age and number of contacts (even genders separately) with a 95% CI. The incidence rate was calculated for individual regions and also its districts, then for whole periods and its years separately. ANOVA analysis was used to compare statistically significant differences between the regions. During the application of ANOVA analysis, the p-value of statistical significance used for calculations was 0.01. ANOVA was used to compare incidence rate differences/specific incidence rate in individual regions for STIs, individual infections, gender, average age and three defined age groups (which corresponded with those defined by the Czech Statistical Office: 0–14, 15–64 and 65+). The incidence as well as specific incidence rates were applied to a population of 100 thousand. For a more detailed analysis of the similarities between these regions, the unpaired T-test was applied between the individual regions and each other. Figures regarding incidence rate for STIs, individual infections and specific incidence rate for gender and defined age groups were included in the T-test analysis. The T-test implementation was preceded by F-test to analyse the congruent variance. The result of the F-test defined whether the given variable will be analysed with the help of an unpaired T-test with equal variance or an unpaired T-test with unequal variance.
RESULTS
The main aim of this study was to find out whether the three selected regions differ from each other in terms of the occurrence of sexually transmitted infections. The basic idea of the occurrence of sexually transmitted infections is shown in Table no. 1 where we can observe the numbers and ratios of individual variables and in some cases also the indicator of incidence rate and average values in quantitative variables (for example the age, number of contacts). In the examined period, the highest incidence rate was reached in the CCP (398.93) where it was 3x higher than in the other two regions (103.98 in PLS and 109.43 in CBR). The average age in all regions was between 32 and 34, the highest of which was in the Pilsen region (33.78, 95 % CI 32.74–34.82). This region also had the highest average age of men (34.41) and women (32.88). In all regions, the average age of women was lower than for men. In all regions there were more men than women reported to be STI positive, from which the highest ratio was recorded in the Capital City of Prague region (75.0% of men). In contrast, the most balanced ratio was recorded in the Pilsen region (58.7% men). From the perspective of ethnicity/ nationality, the ratio of Czechs (78.7 % vs. 79.8 %) was quite balanced in two regions (CCP and CBR). On the other hand, the Pilsen region represented the lowest distribution of Czechs (69.7%) and it was also in this region that the highest ratio of Roma was recorded (4.4%). When comparing the family status, all regions have most representatives (more than 50% of all cases) in the “single” category. In all regions, the “married” made up the second highest representation in this category; the highest ratio of which (around 1/5 of all cases) was in the Pilsen region. From the perspective of education, in two regions (CCP and CBR) the highest ratio was represented by individuals who graduated high school with a diploma (in both cases more than 40%) whereas in the Pilsen region, it was individuals who graduated high school without a diploma (around 35%). We notice similarities between the CCP and CBR also in terms of economic activity where the most representation is by the employed or self-employed, in both cases the ratio being higher than 60%. In the PLR, this category also made up the highest ratio, even if less than ½ of the cases, whereas in this category there was also a high ratio of unemployed (24.4% in comparison to 16.1% in CCP and 16.9% in CBR). We can observe bigger differences in all regions in the varying “way of transfer” where the highest ratio is reached by heterosexual intercourse, though it differed between regions. In CCP, the transfer ratio of “heterosexual contact” was 59.9%, 79.7% in PLR and then 70.7% in CBR. This variable was compensated mainly by homosexual transfer in all regions. For the occurrence of infection variable, the most dominant in all regions was “for the first time in their life”; the highest ratio of reinfection was reported by CCP (17.7%). The most common situation in CCP and CBR when the infection was identified was when the patient would go get tested due to typical difficulties; in the case of PLR, the illness was most often identified randomly. Screening made up in the regions 13.1% to 17.4%, representing the third most important method of detecting STIs.
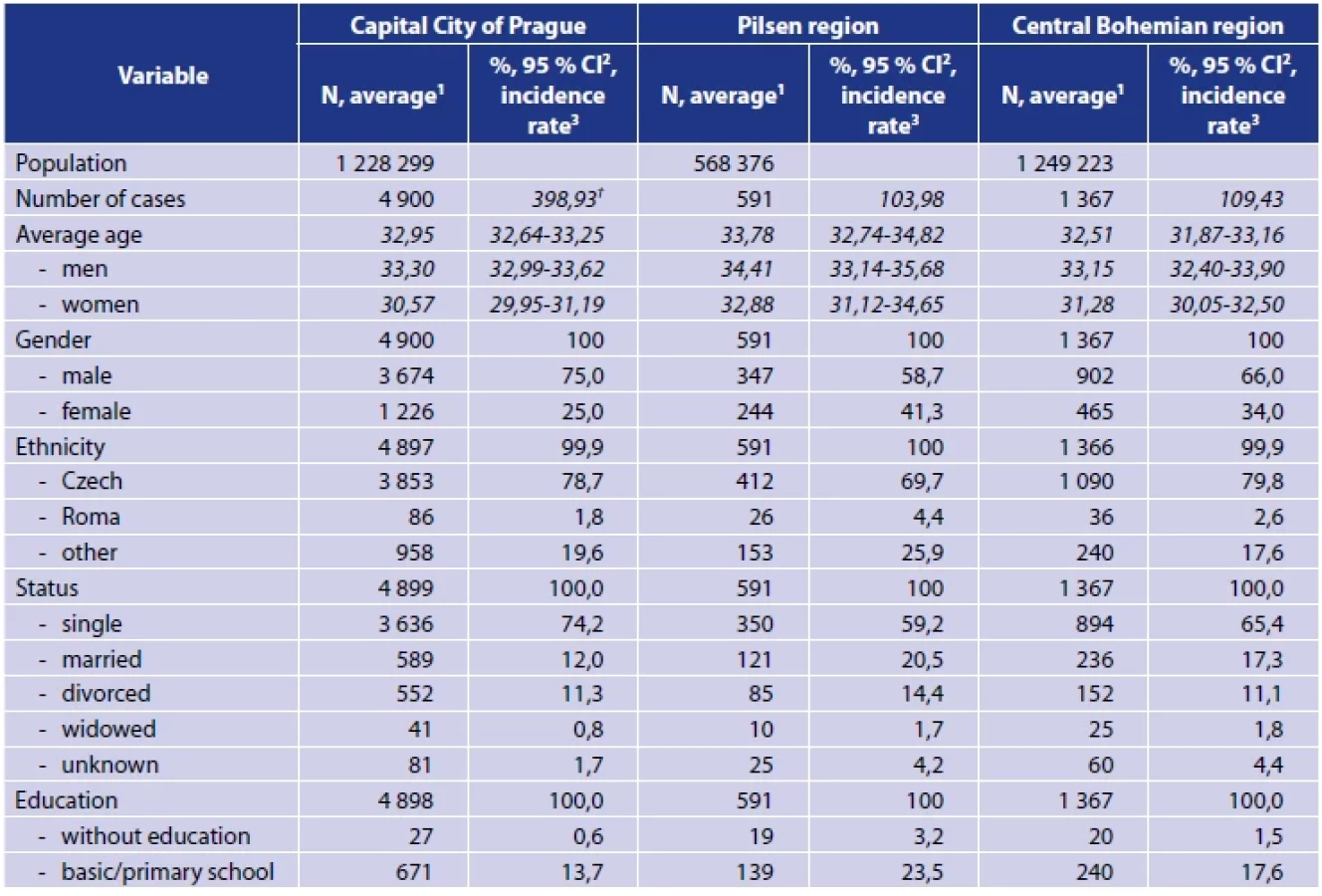

2 The values presenting the reliability interval are presented in cursive in the table and always include intervals.
3 The values presenting the incidence rate (†) are written in cursive in the table and do not include the intervals in a population of 100 thousand.
One of the last examined variables was the patient’s HIV status, which was provided in most cases, although it wasn’t possible to find this status for 21.4% of patients in CBR, 19.5% in CCP and 11.3% in PLS; alternatively, the diagnosis was not indicated. HIV coinfection was reported for 5.5% of patients in CCP and 5.3% in CBR and even less in PLS: 3.9%. Women were examined for pregnancies, whereas in all regions they were examined if STI positive. The most pregnant women with some STI were reported in PLS (17.2%) and the least in CCP (11.4%). A very important piece of information is whether the source of the infection was managed to be identified. While this variable was not found in CCP, the source was successfully identified in PLS (28.9%) and CBR (22.1%). The last variable, “average number of contacts” was also significantly different between regions. The highest average number of contacts was reported in PLS (1.27 per case) and the lowest in CCP (0.52). In all regions, a higher number of contacts was reported for women than men.
Within the frame of individual STIs, the status of CCP was once again very different from the other regions regarding all three infections of focus (syphilis, gonorrhoea, lymphogranuloma venereum). The biggest difference is reported for gonorrhoea, which’s incidence rate in CCP was 223.72 cases per 100 thousand, which is roughly 4x more than in other regions. In the case of syphilis, this difference had a circa 3x lower incidence rate. In the case of LGV, this difference was even bigger, but thanks to the low case numbers it isn’t suitable to compare the incidence rates. The incidence rate and other values in relation to individual infections within the regions are listed in Table no. 2. It is evident from the results that syphilis differs from gonorrhoea in all regions with its higher average age of 36 whereas for gonorrhoea it is around 30. An even bigger difference in average age during diagnosis is for men. For syphilis, the average age is 37.01 in CCP, 39.36 in PLS and 36.54 in CBR whereas for gonorrhoea it is 30.98% in CCP, 30.63 in PLS and 30.46 in CBR – the situation for women is similar. Major differences can be noted in the ratio of men with syphilis: 72.8% in CCP in comparison to 62.1% in CBR and even less in PLS with 47.4%, from which one can deduce that men formed the higher ratio of individuals diagnosed with syphilis. In comparison, the difference is relatively small for gonorrhoea – the values in all three regions are between 69.3 and 76.5 %, the highest ratio of men being once again in CCP. Same situation arose with LGV in all regions of focus, as it was only reported in men. The main way of transfer for syphilis and gonorrhoea was heterosexual intercourse. However, the highest number of homosexually transmitted infection was reported for both infections in CCP (syphilis up to 43.6%, gonorrhoea 36.8%) whereas in the other two regions this ratio was significantly less for syphilis (15.7% in PLS, 23.8% in CBR) and gonorrhoea (11.5% in PLS and 24.2% in CBR). The transfer of LGV differed; it was reported to be only through homosexual intercourse in CCP and CBR whereas in PLS it was only through heterosexual contact.
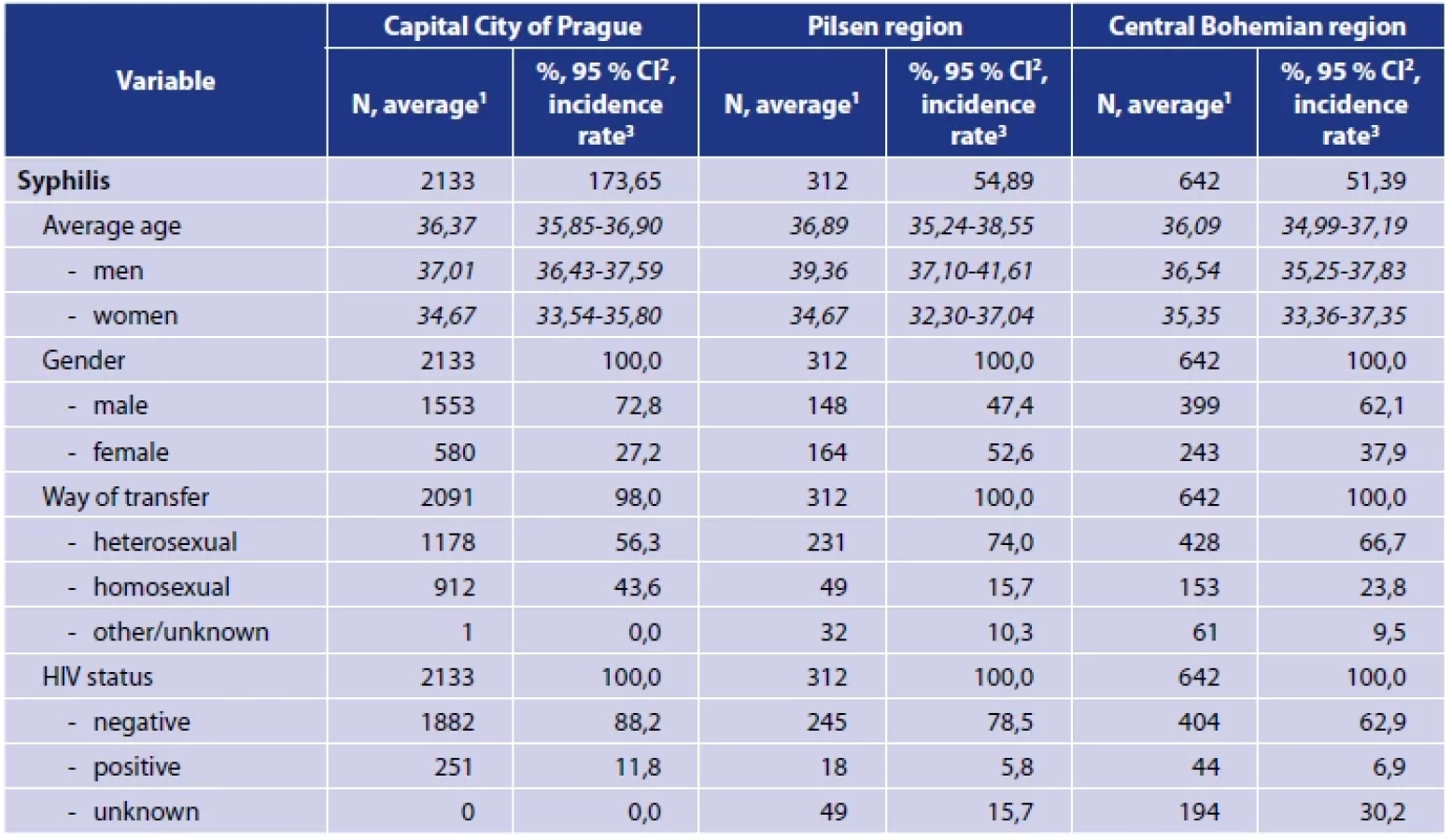


2 The values presenting the reliability interval are presented in cursive in the table and always include intervals.
3 The values presenting the incidence rate are written in cursive in the table and do not include the intervals in a population of 100 thousand.
We can also observe in the obtained data the occurrence of HIV coinfection that most often appears with LGV in 94.7% of cases in CCP, 100% in the CBR, but then in 0% of cases in PLS. The HIV coinfection also appears more often with syphilis than gonorrhoea in all regions. The source of infection was successfully identified more often for gonorrhoea than syphilis: 33.5% vs. 25.0% in PLS and 23.4% vs. 20.7% in CBR. In the case of the last infection, LGV, the source of infection wasn’t successfully identified even for one patient.
From the perspective of examining the epidemical situation, the incidence rate is a very important attribute that testifies the number of newly diagnosed STI cases. The development of this indicator in all regions is provided in Appendix no. 1. In all tracked years, the incidence rate was the highest in the Capital City of Prague region (always more than 40 cases in a population of 100 thousand). In contrast, the indicator reaches its lowest values in the Pilsen region almost throughout the selected period of study. The development of the incidence rate has been progressive in all regions, despite occasional oscillation. In the last column of the table one can observe the incidence rate for the entire period. The highest values of the incidence rate were recorded in CCP in the 9th district of administration, which represents the neighbourhoods Vysočany, Hrdlořezy, Střížkov, Hloubětín, Libeň and Malešice. This administrative district represents the only district where the incidence rate reached values higher than 100 cases per 100 thousand. In the Pilsen region, the highest incidence rates between 2006 and 2013 were in the Domažlice and City of Pilsen districts, even though for the entire period in observation the value was always higher in the first one.


In the last region of Central Bohemia, the highest incidence values were very similar in three districts (Kladno, Mladá Boleslav and Prague-West) with more than 140 cases per 100 thousand. In the Central Bohemian and City of Prague regions, the highest incidence rate was reported at the end of the observed period in 2013, whereas in Pilsen the highest value of this variable was reached in 2007.
The ANOVA analysis was used to compare differences between selected variables between individual regions; the results are summarised in Table no. 3. ANOVA was implemented for incidence rate values of these variables: STIs, individual infections, gender, average age and for individual age groups as defined by the Czech Statistical Office. The p-value of statistical significance used for calculations was set at 0,01. Most variables were even at this p-value statistically significant with exception of the variables LGV (p-value 0.068), age group 0–14 (p-value 0.062) and age group 65+ (p-value 0.025).

2 p-value was calculated for the value 0,01
Statistically major differences between regions for incidence rate of all STIs were completely verified, the biggest difference being reported for CCP where this value was 3x higher than for the other two regions. The last table, Table no. 4, demonstrates comparisons between individual regions, which detects statistically important differences between these regions separately. We see that statistically important differences are evident mainly between Prague and the other two regions, but not between the Pilsen and Central Bohemia regions. The regions did not have significant differences between each other when it came to the LGV infection, which can be partly explained by a low value of the incidence rate. Likewise, the age groups 0-14 and 65+ are without statistically significant differences between all three regions, which can also be due to the influence of low value of the incidence rate. In contrast, major statistically significant differences were recorded in the age group 15–64 for all three regions; it is also this age group that had the most cases.

On the level of statistical significance, it has not been possible to identify major differences between individual regions concerning average age.
DISCUSSION
This study focussing on the epidemiological comparison of the development of sexually transmitted infections in three regions is unique from the perspective of how individual data was worked with. However, this data was provided in different time periods and therefore this study only concerns data obtained for all three regions for the 2006–2013 time-period, even though some regions could provide data even until 2018. Considering the time-consuming processes of transcribing screening reports as a means of extracting information while preserving the individual character for the data and then also about the legal regulations necessary to obtain access to the data, the time perspective appears to be one of the study’s biggest limitations. The retrospective character of this study does not offer recent insights into the problematic of development of sexually transmitted infections, despite however providing valid and relevant information about the occurrence of this group of infections in three regions in the Czech Republic in the selected period.
The study includes data for altogether 6 858 cases of STIs in the regions of the Capital City of Prague, Pilsen and Central Bohemia. During the period of focus, the incidence rate reached the highest values in the Capital City of Prague region (398.93 per 100 thousand). Conversely, the lowest values were recorded in the Pilsen region (103.98 per 100 thousand). In terms of individual years, the highest incidence value was reported in the year 2013 in the CCP and CBR regions, then in PLS in the year 2007. From the perspective of the incidence rate indicator, the regions differ from each other on a statistically significant level for syphilis and gonorrhoea. The same applies to the specific incidence rate for gender and then from the perspective of age groups only the 15–64 group which was the most numerous. There is also statistical similarity between the regions, mainly between PLS and CBR that do not differ from each other in most observed variables, although they did differ considerably in comparison to CCP. This fact demonstrates that in core areas, the epidemiological situation of STIs significantly differs from areas that have a more peripheral character. The individual regions did not significantly differ from each other in variables that were represented by low number of cases (LGV cases and the 0–15 and 65+ age groups). From this perspective it is perhaps more suitable to use a statistic method that better reflects comparative groups of different sizes, such as Poisson regression.
In terms of individual infections, the highest incidence rate was for gonorrhoea (MKS-10 A54), found in two regions of focus (223.72 in CCP and 57.8 in CBR per 100 thousand). This infection was also recorded for individuals of younger average age (29.34–30.25) than other STIs, which corresponds to the situation in the country [8]. However, Jakopanec [9] shows in his 2009 study that this data can be misleading, especially because this illness most commonly passes symptomatic for men and that at the same time, preventative programs target more the young, which can distort the average age of the infected. When examining the specific incidence ratio for gonorrhoea, we can notice the difference between CCP and the remaining two regions that do not have considerable statistical differences between each other. Most cases in the study were composed of men, which was the situation in all regions (69,3% in CBR and up to 76,5% in CCP), which corresponds to the all-European trend [7]. As stated by the ECDC (2018) [7] or Jakopanec (2009) [9], a significant ratio of these men fell into the MSM/homosexual categories. The highest proportion was reported in the CCP with 36.8% of all cases (according to ECDC, 2018, up to 48% in the EU) whereas the lowest was in PLS with 11.5%. However, even this data (concerning the epidemy within the scope of MSM) is necessary to be interpreted carefully. As reminded in the study by Kirkcaldy et al. (2019) [18], data about gonorrhoea for MSM is limited in most countries due to insufficient surveillance, alternatively in consequence of difficult selection of population thanks to stigmatisation and discrimination. Last but not least, it is also the result of the aforementioned factor of the infection’s symptomatic course in men, which happens quite frequently and potentially also increases the representation of men and MSM.
In this study, the syphilis infection had the second highest incidence rate in two regions, the exception being PLS where gonorrhoea appeared more frequently (incidence rate 54,89 per 100 thousand). Even in the case of this infection, the incidence rate was significantly higher in CCP. The reality that the concentration of syphilis in urban areas was also pointed out in the studies of Hughes et al. (2015) [1] and then Fenton et al. (2008) [4], who adverts its consequential diffusion into suburban and even rural areas. Both of these authors also emphasise the thought of greater focus on MSM for a more complex understanding of the syphilis epidemiological situation. This study also identified a significantly higher ratio of MSM/homosexual means of transfer also in the CCP region, therefore in a purely urban area. Here, homosexual way of transfer formed 43.6% of all cases, whereas men altogether formed 72.8%. In PLS, the ratio of homosexually transferred infections was the lowest (15.7%); the result of the higher ratio of the same means of transmission in the CBR is evidently associated with the physical proximity of CCP. The importance of the MSM population in relation to syphilis is also stated by Zetola, Klausner (2007) [14] who explain that the surge of syphilis in this subpopulation mainly through the disinclination to have safe sex, but they also draw attention to how MSM and majority populations understand safe sex differently. This problematic is similarly interpreted also by Kojima, Klausner (2018) [5] who indicate that syphilis persists in this subpopulation mainly as a consequence of the inclination to have a higher number of sexual partners. Peterman et al. (2005) [19] have presented a similar viewpoint on the problematic, pointing out the more common occurrence of both higher number of sexual partners and anonymous sexual partners in MSM. However, Peterman et al. (2015) [15] have presented in their next work another explanation, saying that the endemically quick spread between MSM could have happened as a consequence of obscuration of this less numerous group by a less populated group by a general decrease of syphilis in the majority population and by the absence of preventative activities in this subpopulation. The average age of this study, however, was higher than in the ECDC report (2019) [3]: 36.09–36.89 in comparison to 25–34 years.
The least common infection was the lymphogranuloma venereum. In this study, its incidence rate was highest in CCP (1,55 per 100 thousand), while the lowest was in PLS (0.18 per 100 thousand). Same as in the rest of Europe, this infection was noticeably different from the others of focus. Thanks to the low number of positive patients, no statistically significant differences were found between the individual regions. According to the ECDC report (2018) [13], men formed 99& of all reported cases; in this study, the situation is very similar as in all regions, men formed 100% of all cases. It was a different situation when it came to mode of transmission where homosexual transference applied to all cases within CCP and CBR, which is associated with the urban character of this infection’s occurrence. However, according to Rawla et al. (2021) [16], the higher ratio of men can be explained with the more frequent and especially earlier manifestation of LGV in the male than female population. LGV is known for its very common association with the HIV infection as LGV-positive patients have 67-100% prevalence of HIV infection [17]. Within the frame of this study, the coinfection of HIV was detected in 94,7% of LGV-positive cases in CCP and 100% in CBR. In his study, Ward et al. (2007) [12] mentions the median age of LGV to be 38+, which corresponds with the average age of LGV positive patients of this study in CCP, where the reported majority with this illness was 38.2 years and then 31.7 years in the case of CBR.
CONCLUSION
This study focussed on sexually transmitted infections in selected regions of the Czech Republic presents results for syphilis, gonorrhoea and LGV, meaning infections falling under mandatory reporting and contained in the system of STIs in the period 2006-2013. The study identified statistically significant differences between integrated regions, mainly between the Capital City of Prague and other two regions. It was Prague that was listed as the region with the highest incidence rate whereas gonorrhoea was indicated as the most common STI (except for the Pilsen region). For the lymphogranuloma venereum illness no statistically significant differences in examined variables were identified, which can be explained mainly by its low occurrence. The study also points out the need for more detailed work that would mainly focus on the problematic of STIs in the MSM subpopulation.
Acknowledgements
At this point I would like to thank the employees and chairmen of the regional public health offices of the Central Bohemia region and Capital City of Prague. My gratitude also goes to the Dermatological clinic of the University Hospital of Pilsen without whose cooperation and willingness this work would not have come into existence.
Do redakce došlo dne 18. 2. 2022.
Adresa pro korespondenci:
Mgr. Jan Carlos Sekera
Papírnická 2809/10
326 00 Plzeň
e-mail: jan.carlos.sekera@gmail.com
Epidemiol Mikrobiol Imunol, 2022; 71(4): 190–202
Zdroje
1. Hughes G, Field N. The epidemiology of sexually transmitted infections in the UK: impact of behavior, services and interventions. Future microbiology, 2015;10(1):35–51.
2. De Waroux OLP, Harris R, Hughes G, et al. The epidemiology of gonorrhoea in London: a Bayesian spatial modelling approach. Epidemiology & Infection, 2014;142(1):211–220.
3. ECDC, Syphilis and congenital syphilis in Europe – A review of epidemiological trends (2007–2018) and options for response [online]. [accessed 2021-08-14]. Available from: https://www.ecdc. europa.eu/en/publications-data/syphilis-and-congenital-syphilis - europe-review-epidemiological-trends-2007-2018.
4. Fenton KA, Breban R, Vardavas R, et al. Infectious syphilis in high-income settings in the 21st century. The Lancet infectious diseases, 2008;8(4):244–253.
5. Kojima N, Klausner JD. An update on the global epidemiology of syphilis. Current epidemiology reports, 2018;5(1):24–38.
6. Institute of Health Information and Statistics of the Czech Republic Registrer of Veneral Diseases [online]. [accessed 2021-01-09]. Available from: https://www.uzis.cz/index. php?pg=regiCBRy-sber-dat--ochrana-verejneho zdravi--regiCBR - pohlavnich-nemoci.
7. ECDC Gonorrhoea – Annual Epidemiological Report for 2018 [online]. [accessed 2021-08-19]. Available from: https://www.ecdc. europa.eu/en/publications-data/gonorrhoea-annual-epidemiological - report-2018.
8. Institute of Health Information and Statistics of the Czech Republic Thematic series – venereal diseases [online]. [accessed 2021-08-20]. Available at: https://www.uzis.cz/index.php?pg= vystupy--tematicke-rady&id=761.
9. Jakopanec I, Borgen K, Aavitsland P. The epidemiology of gonorrhoea in Norway, 1993–2007: past victories, future challenges. BMC Infectious diseases, 2009;9(1):1–11.
10. Stary G, Stary A. Lymphogranuloma venereum outbreak in Europe. JDDG: Journal der Deutschen Dermatologischen Gesellschaft, 2008;6(11):935–939.
11. Diaz A, Ruiz-Alguero M, Hernando V. Lymphogranuloma venereum in Spain, 2005–2015: A literature review. Medicina Clínica (English Edition), 2018;151(10):412–417.
12. Ward H, Martin I, Macdonald N, et al. Lymphogranuloma venereum in the United Kingdom. Clinical infectious diseases, 2007;44(1):26–32.
13. ECDC Lymphogranuloma venereum – Annual Epidemiological Report for 2018 [online]. [accessed 2021-08-12]. Available from: https://www.ecdc.europa.eu/en/publications-data/lymphogranuloma - venereum-annual-epidemiological-report-2018.
14. Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clinical Infectious Diseases, 2007;44(9):1222–1228.
15. Peterman TA, Su J, Bernstein KT, et al. Syphilis in the United States: on the rise?. Expert review of anti-infective therapy, 2015;13(2):161–168.
16. Rawla P, Thandra KC, Limaiem F. Lymphogranuloma Venereum. 2022. In: StatPearls [Internet]. Treasure Island (FL): StatPearl Publishing; 2022. PMID: 30726047.
17. De Vrieze NHN, De Vries HJC. Lymphogranuloma venereum among men who have sex with men. An epidemiological and clinical review. Expert review of anti-infective therapy, 2014;12(6):697–704.
18. Kirkcaldy RD, Weston E, Segurado AC, et al. Epidemiology of gonorrhoea: a global perspective. Sexual health, 2019;16(5):401 – 411.
19. Peterman TA, Heffelfinger JD, Swint EB, et al. The changing epidemiology of syphilis. Sexually transmitted diseases, 2005;32(10):S4–S10.
20. Czech Statistical Office Demographic almanac [online]. [accessed 2021-08-19]. Available from: https://www.czso.cz/csu/ czso/casova_rada_demografie.
Štítky
Hygiena a epidemiológia Infekčné lekárstvo MikrobiológiaČlánok vyšiel v časopise
Epidemiologie, mikrobiologie, imunologie

2022 Číslo 4
- Parazitičtí červi v terapii Crohnovy choroby a dalších zánětlivých autoimunitních onemocnění
- Očkování proti virové hemoragické horečce Ebola experimentální vakcínou rVSVDG-ZEBOV-GP
- Koronavirus hýbe světem: Víte jak se chránit a jak postupovat v případě podezření?
Najčítanejšie v tomto čísle
- Nosičství Neisseria meningitidis u nastupujících mladých vojenských profesionálů v období pandemie onemocnění covid-19
- Molekulární určení genotypu izolátů Streptococcus agalactiae s netypovatelným sérotypem, Česká republika, 2008–2020
- Acute kidney injury requiring renal replacement therapy due to Clostridioides difficile infection in a 15-year-old boy
- Comparing the epidemiological situation of selected sexually transmitted infection in three Czech regions between 2006 and 2013