
Exudative Retinal Detachment in Preeclampsia. Case Reports
Exudative Retinal Detachment in Preeclampsia. Case Reports
Preeclampsia, eclampsia and HELLP syndrome are serious pregnancy-related complications associated with significant morbidity and mortality. These pathological conditions are related to placental dysfunction, systemic endothelial dysfunction and various clinical and biochemical abnormalities. Exudative retinal detachment as a rare but clinically significant ophthalmologic complication of preeclampsia occurs in 0.2–2% of cases, more frequently affecting primigravidas and often presenting bilaterally. This article presents two case reports of patients with preeclampsia complicated by exudative retinal detachment. The first case describes a 22-year-old primigravida at 35 weeks of gestation with preeclampsia, bilateral visual impairment and exudative retinal detachment. The second case involves a 38-year-old primigravida at 31 weeks of gestation with preeclampsia and incompletely expressed HELLP syndrome, in whom visual impairment and unilateral exudative retinal detachment developed after delivery. In both patients, the exudative retinal detachment was resolved and visual acuity improved within a month after delivery and with stabilization of blood pressure.
Klíčová slova:
Preeclampsia – HELLP syndrome – exudative retinal detachment – visual complications of pregnancy
Authors:
Vladimír Kováč 1; Michaela Leštachová Viková 1; Petra Bačová 1; Jana Štefaničková 2,3; Mária Praženicová 1; Ladislav Jančo 1
Authors place of work:
II. Clinic of Ophthalmology SZU, FNsP F. D. R. Banská Bystrica, Slovakia
1; Clinic of Ophthalmology LFUK a UN Bratislava, Slovakia
2; Oftalmocentrum Betliarska Euromedix, Bratislava, Slovakia
3
Published in the journal:
Čes. a slov. Oftal., 81, 2025, No. Ahead of Print, p. 1-6
Category:
Kazuistika
doi:
https://doi.org/10.31348/2025/34
Summary
Preeclampsia, eclampsia and HELLP syndrome are serious pregnancy-related complications associated with significant morbidity and mortality. These pathological conditions are related to placental dysfunction, systemic endothelial dysfunction and various clinical and biochemical abnormalities. Exudative retinal detachment as a rare but clinically significant ophthalmologic complication of preeclampsia occurs in 0.2–2% of cases, more frequently affecting primigravidas and often presenting bilaterally. This article presents two case reports of patients with preeclampsia complicated by exudative retinal detachment. The first case describes a 22-year-old primigravida at 35 weeks of gestation with preeclampsia, bilateral visual impairment and exudative retinal detachment. The second case involves a 38-year-old primigravida at 31 weeks of gestation with preeclampsia and incompletely expressed HELLP syndrome, in whom visual impairment and unilateral exudative retinal detachment developed after delivery. In both patients, the exudative retinal detachment was resolved and visual acuity improved within a month after delivery and with stabilization of blood pressure.
Keywords:
HELLP syndrome – preeclampsia – exudative retinal detachment – visual complications of pregnancy
INTRODUCTION
Preeclampsia, eclampsia and HELLP syndrome are serious pregnancy-related complications, which significantly influence the morbidity and mortality of mothers and newborn infants. These conditions are closely related to placental dysfunction and systemic endothelial dysfunction, which lead to several clinical and biochemical abnormalities. Preeclampsia is defined as hypertension (≥ 140/90 mmHg) occurring after the 20th week of pregnancy in combination with proteinuria (≥ 300 mg/24 hours), and with generalized edema or with manifestations of organ damage without proteinuria [1]. The incidence of this disease is between 3 and 7% of all pregnancies, and it develops predominantly in the first pregnancy or in women expecting twins [2]. It occurs upon a background of impaired vascular development of the placenta, and causes systemic endothelial dysfunction and microangiopathy through the production and distribution of anti-angiogenic factors into the blood circulation of the mother [2]. Hypertension, diabetes, obesity, renal disorders, multiple pregnancy, hormonal contraceptive use history, low or high age, connective tissue diseases, thrombotic vascular diseases, family history of preeclampsia and in vitro fertilization are further risk factors of preeclampsia occurrence [1,2]. Preeclampsia may lead to serious complications such as placental abruption, intrauterine growth restriction and premature birth [3]. Eclampsia, which is considered the most serious form of preeclampsia, is manifested in the occurrence of generalized tonic-clonic seizures in patients with preeclampsia. The mechanisms of origin of eclampsia incorporates cerebrovascular changes such as vasospasm, edema and hemorrhage, leading to neurological symptoms [1]. HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count) represents a serious variant of preeclampsia which is distinguished by hemolysis, hepatic enzymes increase and thrombocytopenia. The incidence of HELLP syndrome is within the range of 0.5% to 0.9% of all pregnancies, and occurs in approximately 10–20% of cases of preeclampsia [4]. The clinical manifestation includes pain in the epigastrium or right hypochondrium, nausea, vomiting and general weakness. HELLP syndrome is associated with an increased risk of disseminated intravascular coagulation (DIC), hepatic rupture and acute renal failure [5].
Ophthalmological complications of preeclampsia, eclampsia or HELLP syndrome include changes in retinal perfusion, optic nerve papilledema, central serous chorioretinopathy and exudative retinal detachment [6,7]. Exudative retinal detachment ranks among rare but clinically serious complications, and is characterized by an accumulation of fluid in the subretinal space, which occurs as a consequence of the blood-retinal barrier integrity breach. This process is potentiated by endothelial dysfunction, deteriorated autoregulation of the choroidal blood vessels and pronounced changes in choroidal perfusion. Hemodynamic changes lead to choroidal ischemia and subsequent fluid infiltration across the Bruch’s membrane into the space between the retina and the retinal pigment epithelium [8]. In this article we present case reports of two female patients with preeclampsia with exudative retinal detachment, one of which had incompletely expressed HELLP syndrome.
Case report no. 1
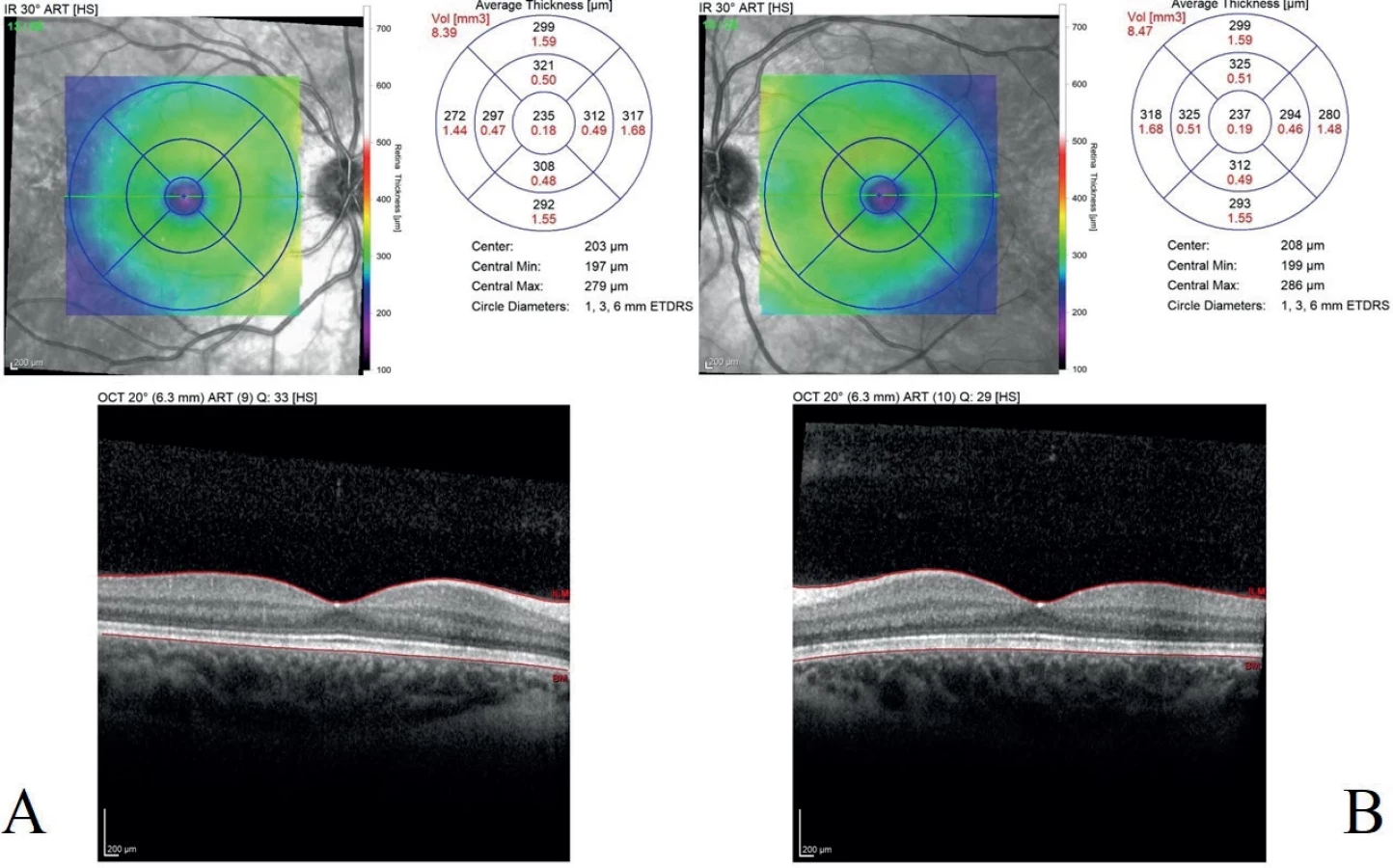
A 22-year-old primigravida in the 35th week of pregnancy came to our central reception for an examination due to raised blood pressure values of 180/110 mmHg, which up to that point had been compensated (during pregnancy), as well as vomiting, bilateral tumescence of the lower and upper limbs and deterioration of vision. In her personal medical history, the patient had gestational hypertension, otherwise her personal anamnesis was without any remarkable features. The patient was hospitalized due to severe preeclampsia, and that night she gave birth by caesarian section. The laboratory parameters demonstrated presence of leukocytosis 14.1*109/l (norm 4.0–10.0), microcytic anemia – erythrocytes 3.72 *1012/l (norm 4.20–5.40), raised level of uric acid 421.0 umol/l (norm 154.7–357.0), reduced overall proteins 49.0 g/l (norm 66.0–83.0), reduced albumin 24.0 g/l (norm 35,0–52,0), raised level of AST 0.78 ukat/l (norm 0.00–0.60), raised ALP 4.41 ukat/l (norm 0.55–1.63), raised LD 5.30 ukat/l (norm 0.00–4.12) and raised CRP 19.68 mg/l (norm 0.00–5.00). It was not possible to determine the values of the blood coagulation parameters due to heavy hemolysis of the sample in question. The morning after giving birth the patient was examined by an ophthalmologist. At the ophthalmological examination, best corrected visual acuity (BCVA) in the right eye was 0.4, in the left eye 0.9. The finding was physiological on the anterior segment of the right and left eye. On the posterior segment of the right eye we found numerous deposits of exudative retinal detachment with cotton wool spots in the macular region of the retina, and on the posterior segment of the left eye we also found a deposit of exudative retinal detachment in the macular region, see Figure 1A, B. OCT examination of the macula of the right and left eye showed subretinal fluid, see Figure 2A, B. Based on medical history and the ocular finding we determined a diagnosis of preeclampsia induced bilateral retinal detachment. Blood pressure compensation was recommended to the attending gynecologist, and local treatment was commenced with non-steroidal anti-inflammatory agent Bromfenac 0.9 mg/ml drops 2x per day bilaterally. Two days after the initial examination BCVA in the right eye was 1.0, in the left eye it had deteriorated to 0.7. We are unable to explain this deterioration of visual acuity in the left eye, and we assume that it occurred after the initial examination due to persistent exudative retinal detachment. The OCT examination demonstrated partial absorption of the subretinal fluid bilaterally. At a follow-up examination one month after birth BCVA in both the right and left eye had improved to 1.0, fundoscopy showed no signs of exudative retinal detachment bilaterally, and OCT examination of the macula of the right and left eye proved that the subretinal fluid had been completely absorbed, see Figure 3A, B. Further follow-up observation of the patient continued at the local ophthalmology clinic.


Case report no. 2
A 38-year-old primigravida in the 31st week of gestation with fetoplacental insufficiency and polyhydramnios, with suspected atresia of the esophagus of the fetus and suspected preeclampsia was admitted to a gynecological clinic. The patient’s personal medical history showed gestational hypertension without proteinuria, bronchial asthma, sinus tachycardia without structural cardiac abnormalities and without an image of heart failure, with minimal pericardial effusion under observation. Upon admittance, blood pressure was 190/110 mmHg, there was bilateral tumescence of the lower limbs, the laboratory parameters showed raised fibrinogen level of 3.59 g/l (norm 1.50–3.50), raised leukocytes 12.4*109/l (norm 4.0–10.0), reduced erythrocytes 3.80*1012/l (norm 4.20–5.40), reduced overall proteins 55.0 g/l (norm 66.0–83.0), reduced albumin 31.0 g/l (norm 35.0–52.0), raised AST 4.24 ukat/l (norm 0.00–0.60), raised ALT 2.89 ukat/l (norm 0.00–0.60) and raised LD 8.80 ukat/l (norm 0.00–4.12). At the initial ophthalmological examination BCVA was 1.0 bilaterally, and since anterior and posterior segment had physiological findings no OCT examination was conducted. During the course of hospitalization, proteinuria and thrombocytopenia of 47*109/l (norm 140–400) progressively developed, and in combination with the already present increase of hepatic parameters the condition was concluded as incompletely expressed HELLP syndrome. As a result the patient was indicated for birth by cesarian section. The day after delivery the patient began to complain of vision deterioration and blurring in the right eye. At a follow-up ophthalmological examination 4 days after the initial examination and one day after birth we observed a deterioration of BCVA in the right eye to the level of 0.4. While anterior segment of the right eye was physiological, high exudative retinal detachment was present on the ocular fundus of the right eye, localized in the macular region, see Figure 4. OCT examination of the macula of the right eye confirmed high serous retinal detachment, see Figure 5. In the left eye BCVA was 1.0, the finding on the anterior and posterior segment and on the OCT examination of the left eye was physiological. Based on medical history and the ocular findings we determined a diagnosis of exudative retinal detachment in the right eye induced by preeclampsia and incompletely expressed HELLP syndrome. Local treatment with Nepafenac 1% drops 3x per day was administered. At subsequent follow-up examinations there was a progressive reduction of exudative retinal detachment and an improvement of visual acuity in the right eye to the level of 0.8. At a follow-up after one month, BCVA in the right eye was at the level of 1.0, exudative retinal detachment was completely absorbed on the ocular fundus, which we also confirmed by OCT examination of the macula, see Figure 6. We kept the patient under observation for 2 years, during which BCVA was maintained at the level of 1.0, the finding on the anterior and posterior segment was physiological bilaterally. At the last examination, the patient was in the 30th week of pregnancy, the ophthalmological finding was physiological bilaterally, and the patient no longer manifested preeclampsia or HELLP syndrome, or associated exudative retinal detachment, see Figure 7.




DISCUSSION
Preeclampsia induced exudative retinal detachment is found in 0.2–2% of cases [9], in which the standard manifestation is bilateral (89%), it is more common in primigravidas (60%) and usually diagnosed after delivery (69%). If HELLP syndrome is also present in women with preeclampsia or eclampsia, the chance of occurrence of exudative retinal detachment is 7x higher [10]. A number of theories exist concerning the mechanism of origin of exudative retinal detachment in preeclampsia. The preferred theory is terminal arteriolar vasospasm of the choroid with subsequent choroidal ischemia, damage to the retinal pigment epithelium, endothelial dysfunction and damage to the outer blood-retinal barrier [11,12]. The subsequent infiltration of proteins and fluids from the choriocapillaris into the subretinal space causes exudative retinal detachment. The onset of choroidal ischemia may be potentiated in HELLP syndrome by the hemolysis of red blood cells and subsequent capillary obstruction [10]. Endothelial dysfunction is directed by anti-angiogenic factors such as SFlt-1 (soluble Fms-like receptor tyrosine kinase-1), which together with vasospasm have been demonstrated to be a part of the pathophysiology of preeclampsia [13].
Patients typically experience suddenly occurring blurring or loss of vision, blind spots in the visual field or change of color perception. In the case of ongoing pregnancy, upon suspicion of exudative retinal detachment caused by preeclampsia or eclampsia early delivery is recommended. In the case that the condition is diagnosed postpartum, compensation of blood pressure is recommended. In most cases, exudative retinal detachment does not require surgical treatment and has a tendency to reabsorb within 12 weeks of the onset of the symptoms [14]. In our patients, exudative retinal detachment was absorbed and BCVA improved to 1.0 within one month of the onset. After delivery and blood pressure compensation BCVA has a tendency to improve to its former level before the onset of exudative retinal detachment in the majority of the published cases, although a case has also been described in which BCVA remained permanently on the level of practical blindness [15]. In some cases of exudative retinal detachment in preeclampsia, the appearance of the retinal pigment epithelium lesions has been described, which persist also after the reabsorption of the subretinal and intraretinal fluid [16,17], though this did not apply to our two patients. A precondition for the appearance of these lesions is ischemia of the choriocapillaris, and the authors Ledesma-Gil and Smith, in their commentary on the article Serous retinal detachment in preeclampsia and malignant hypertension by Lee et al., reflect upon the similarities with age-related macular degeneration. After a comparison of the images from indocyanine green angiography, where it is possible to see delay and numerous defects of the choroidal filling in the early phases of both diagnoses, they consider this to represent convincing evidence that chronic choriocapillaris insufficiency is the main pathomechanism also in the origin of subretinal drusenoid deposits in patients with age-related macular degeneration [16,18]. A question remains as to why unilateral preeclampsia induced exudative retinal detachment is observed, as in Case Report No. 2, given that preeclampsia is a systemic pathology. It is possible that the unilateral pathology is merely the first manifestation of a process which, if not identified and treated in time, would also appear in the other eye. Several theories exist as to why preeclampsia predominantly affects primigravidas, including worse adaptation of the mother’s immune system to the presence of the fetus and placenta, which have foreign antigens for the mother’s immune system, as lack of previous exposure to the father’s antigens [19], disorders of vascular remodeling in the placenta, which results in insufficient blood supply, higher placental stress, oxidative damage or genetic and epigenetic factors, which in the first pregnancy trigger different gene expressions in the tissues of the mother and the placenta, or a combination thereof [20]. In our patient in Case Report no. 2, preeclampsia also occurred in the first pregnancy, whereas the second pregnancy was without any such complications.
CONCLUSION
Exudative retinal detachment in preeclampsia represents a significant risk for visual acuity. In the case of timely diagnosis and correct treatment, which includes early delivery and compensation of blood pressure, the prognosis for visual acuity is favorable, which was presented also in our two patients from the case reports. Last but not least, it is necessary to emphasize the significance and importance of interdisciplinary cooperation of an ophthalmologist with a gynecologist. It is only through cooperation that we can protect the health and sight of our patients.
Zdroje
- Perloff D. Hypertension and pregnancy-related hypertension. Cardiol Clin. 1998; 16 : 79-101. doi: 10.1016/s0733-8651(05)70386-6
- Al-Jameil N, Khan FA, Khan MF, Tabassum H. A Brief Overview of Preeclampsia. J Clin Med Res. 2014 Feb; 6(1):1-7. doi: 10.4021/jocmr1682w
- American College of Obstetricians and Gynecologists (ACOG). Hypertension in pregnancy. Obstet Gynecol. 2013;122(5):1122-1131. doi: 10.1097/01.AOG.0000437382.03963.88
- Haram K, Svendsen E, Abildgaard U. The HELLP syndrome: Clinical issues and management. A review. BMC Pregnancy Childbirth. 2009; 9 : 8. doi.org/10.1186/1471-2393-9-8
- Magee LA, Smith GN, Bloch Ch, et al. Guideline No. 426: Hypertensive Disorders of Pregnancy: Diagnosis, Prediction, Prevention, and Management. J Obstet Gynaecol Can. 2022 May;44(5):547 - 571. doi: 10.1016/j.jogc.2022.03.002
- Tranquilli AL, Dekker G, Magee L, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014;4(2), 97-104. doi: 10.1016/j.preghy.2014.02.001
- Cunningham FG, et al. Williams Obstetrics. 25th edition. (United States of America) McGraw-Hill Education; 2018.
- Hayreh SS. Pathogenesis of visual field defects in hypertensive choroidopathy: Experimental study. Arch Ophthalmol. 2011; 129(6):812-819.
- Khallouli A, Choura R, Saidane R, et al. Bilateral exudative retinal detachment in HELLP syndrome, first description in North Africa: A case report. PAMJ 2021, 39, 6 doi:10.11604/pamj-cm.2021.6.39.25913
- Garcia PV, Ortega-Paz L. Retinal Detachment in association with pre-eclampsia, eclampsia, and HELLP syndrome. Int J Gynaecol Obstet. 2011 Sep; 114(3); 223-225. doi: 10.1016/j.ijgo.2011.04.003
- Song YA, Kinouchi R, Ishiko S, Fukui K, Yoshida A. Hypertensive choroidopathy with eclampsia viewed on spectral-domain optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2013;251;2647-2650. doi: 10.1007/s00417-013-2462-9
- Querques L, Querques G, Loperfido F, Lattanzio R, BandelloF. Enhanced depth imaging optical coherence tomography findings associated with serous retinal detachment in preeclampsia. Arch Gynecol Obstet. 2014;289;457-459. doi: 10.1007/s00404-013-2966-x
- Phipps EA, Thadhani R, Benzing T et al. Preeclampsia: pathogenesis, novel diagnostics and therapies. Nature rev Nephrol. 2019; 15 : 275-289. doi: 10.1038/s41581-019-0119-6
- Benlghazi A, Bouhtouri Y, Belouad M, et al. Bilateral serous retinal detachment in pre-eclampsia a rare but favorable complication: case report. Oxf Med Case Reports. 2023 Oct 23;2023(10):omad109. doi: 10.1093/omcr/omad109
- Chen KH, Chen LR. Bilateral retinal detachment with subsequent blindness in a pregnant woman with severe pre-eclampsia. Taiwan J Obstet Gynecol. 2013; 52 : 142-144. doi: 10.1016/j.tjog.2012.05.001
- Lee CS, Choi EY, Lee M, Kim H, Chung H. Serous retinal detachment in preeclampsia and malignant hypertension. Eye (Lond). 2019 Nov;33(11):1707-1714. doi: 10.1038/s41433-019-0461-8
- Munsell MK, Carducci NM, Eton EA. Exudative Retinal Detachment and Ciliochoroidal Effusion in Preeclampsia. J Vitreoretin Dis. 2023 Feb 17;7(3):254-258. doi: 10.1177/24741264221147986
- Ledesma-Gil G, Smith RT. Comment on: „Serous retinal detachment in preeclampsia and malignant hypertension“. Eye (Lond). 2019 Nov;33(11):1818. doi: 10.1038/s41433-019-0514-z
- Dekker GA, Robillard PY. Preeclampsia-an immune disease? An epidemiologic narrative. Explor Immunol. 2021; 1 : 325-340. doi. org/10.37349/ei.2021.00022
- Geldenhuys J, Rossouw TM, Lombaard HA, Ehlers MM, Kock MM. Disruption in the Regulation of Immune Responses in the Placental Subtype of Preeclampsia. Front. Immunol. 2018; 9;1659. doi: 10.3389/fimmu.2018.01659
Štítky
OftalmológiaČlánok vyšiel v časopise
Česká a slovenská oftalmologie

2025 Číslo Ahead of Print
- Pomocné látky v roztoku latanoprostu bez konzervačních látek vyvolávají zánětlivou odpověď a cytotoxicitu u imortalizovaných lidských HCE-2 epitelových buněk rohovky
- Konzervační látka polyquaternium-1 zvyšuje cytotoxicitu a zánět spojený s NF-kappaB u epitelových buněk lidské rohovky
- Dlouhodobé výsledky lokální léčby cyklosporinem A u těžkého syndromu suchého oka s 10letou dobou sledování
- Syndrom suchého oka
- Cyklosporin A v léčbě suchého oka − systematický přehled a metaanalýza
Najčítanejšie v tomto čísle
- Clinical Outcomes of Preserflo MicroShunt versus Trabeculectomy: A Retrospective 6-Month Study
- Choroidal Neovascular Membrane in Pediatric Patients: Long-Term Outcomes of Anti-VEGF Therapy
- Exudative Retinal Detachment in Preeclampsia. Case Reports
- Chorioretinitis Associated with HSV-1 Neuroinfection Following Viral Infection. A Case Report