
Choroidal Neovascular Membrane in Pediatric Patients: Long-Term Outcomes of Anti-VEGF Therapy
Choroidal Neovascular Membrane in Pediatric Patients: Long-Term Outcomes of Anti-VEGF Therapy
Aim: To evaluate the epidemiological data, etiology and clinical characteristics, and to assess the efficacy and safety of intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy in the treatment of choroidal neovascular membrane (CNV) in children and adolescents. The results are compared with data from previously published studies and case reports.
Material and Methods: Retrospective analysis of medical records of patients treated for CNV at the Department of Pediatric Ophthalmology, University Hospital Brno, between January 2015 and April 2025. The cohort consisted of 12 patients, including 7 males and 5 females. All the cases involved unilateral disease; the right eye was affected in 7 patients and the left eye in 5. The mean age at onset was 11.8 years (range: 3–17 years). All underwent a comprehensive ophthalmological examination including optical coherence tomography (OCT); in 7 cases the diagnosis was confirmed by fluorescein angiography. The evaluated parameters included epidemiological data, clinical and morphological characteristics of CNV before and after anti-VEGF therapy. The etiology of CNV in our cohort was as follows: post-inflammatory/post-infectious in 6 cases, idiopathic in 3 cases, and one case each of myopic, post-traumatic, and neoplastic origin. The most common localization was subfoveal. All CNV lesions were classified as classic (type 2).
Results: All patients achieved either anatomical or functional improvement. No ocular or systemic adverse effects related to intravitreal anti-VEGF therapy were observed during the study period.
Conclusion: Early diagnosis and intervention with anti-VEGF therapy show favorable outcomes, including stabilization and remission of the disease. In our cohort, no adverse events or complications associated with intravitreal anti-VEGF administration were recorded. Continued research is essential in order to gain a further understanding of the pathogenesis of pediatric CNV and to optimize treatment strategies in children.
Klíčová slova:
ranibizumab – anti-VEGF – choroidal neovascularization – pediatric CNV – choroidal neovascular membrane in children – secondary CNV
Authors:
Kamila Pavlíková 1; Inka Krejčířová 1; Rudolf Autrata 1; Kateřina Šenková 1; Veronika Matušková 2
Authors place of work:
Department of Pediatric Ophthalmology, University Hospital Brno and, Faculty of Medicine, Masaryk University, Brno, Czech Republic
1; Department of Ophthalmology, University Hospital Brno and Faculty, of Medicine, Masaryk University, Brno, Czech Republic
2
Published in the journal:
Čes. a slov. Oftal., 81, 2025, No. Ahead of Print, p. 1-8
Category:
Původní práce
doi:
https://doi.org/10.31348/2025/33
Summary
Aim: To evaluate the epidemiological data, etiology and clinical characteristics, and to assess the efficacy and safety of intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy in the treatment of choroidal neovascular membrane (CNV) in children and adolescents. The results are compared with data from previously published studies and case reports.
Material and Methods: Retrospective analysis of medical records of patients treated for CNV at the Department of Pediatric Ophthalmology, University Hospital Brno, between January 2015 and April 2025. The cohort consisted of 12 patients, including 7 males and 5 females. All the cases involved unilateral disease; the right eye was affected in 7 patients and the left eye in 5. The mean age at onset was 11.8 years (range: 3–17 years). All underwent a comprehensive ophthalmological examination including optical coherence tomography (OCT); in 7 cases the diagnosis was confirmed by fluorescein angiography. The evaluated parameters included epidemiological data, clinical and morphological characteristics of CNV before and after anti-VEGF therapy. The etiology of CNV in our cohort was as follows: post-inflammatory/post-infectious in 6 cases, idiopathic in 3 cases, and one case each of myopic, post-traumatic, and neoplastic origin. The most common localization was subfoveal. All CNV lesions were classified as classic (type 2).
Results: All patients achieved either anatomical or functional improvement. No ocular or systemic adverse effects related to intravitreal anti-VEGF therapy were observed during the study period.
Conclusion: Early diagnosis and intervention with anti-VEGF therapy show favorable outcomes, including stabilization and remission of the disease. In our cohort, no adverse events or complications associated with intravitreal anti-VEGF administration were recorded. Continued research is essential in order to gain a further understanding of the pathogenesis of pediatric CNV and to optimize treatment strategies in children.
Keywords:
ranibizumab – anti-VEGF – choroidal neovascularization – pediatric CNV – choroidal neovascular membrane in children – secondary CNV
INTRODUCTION
Choroidal neovascular membrane (CNV) is a rare pathology in pediatric patients, which may nevertheless cause serious damage to or even loss of central vision, especially in the case that the lesion is located in the central region of the retina. It differs from CNV that occurs in the older adult population primarily in its etiology, but also in its clinical picture and response to therapeutic interventions [1]. Whereas in older patients the origin of CNV is mostly associated with age-related macular degeneration (ARMD), in children CNV develops secondarily upon a background of another predisposing pathology [2].
CNV forms in newly formed choroidal vessels, which penetrate the Bruch’s membrane into the subretina space or beneath the retinal pigment epithelium (RPE). The initiating factor for the occurrence of CNV is breach of the integrity of the Bruch’s membrane and pathological changes of the RPE [3].
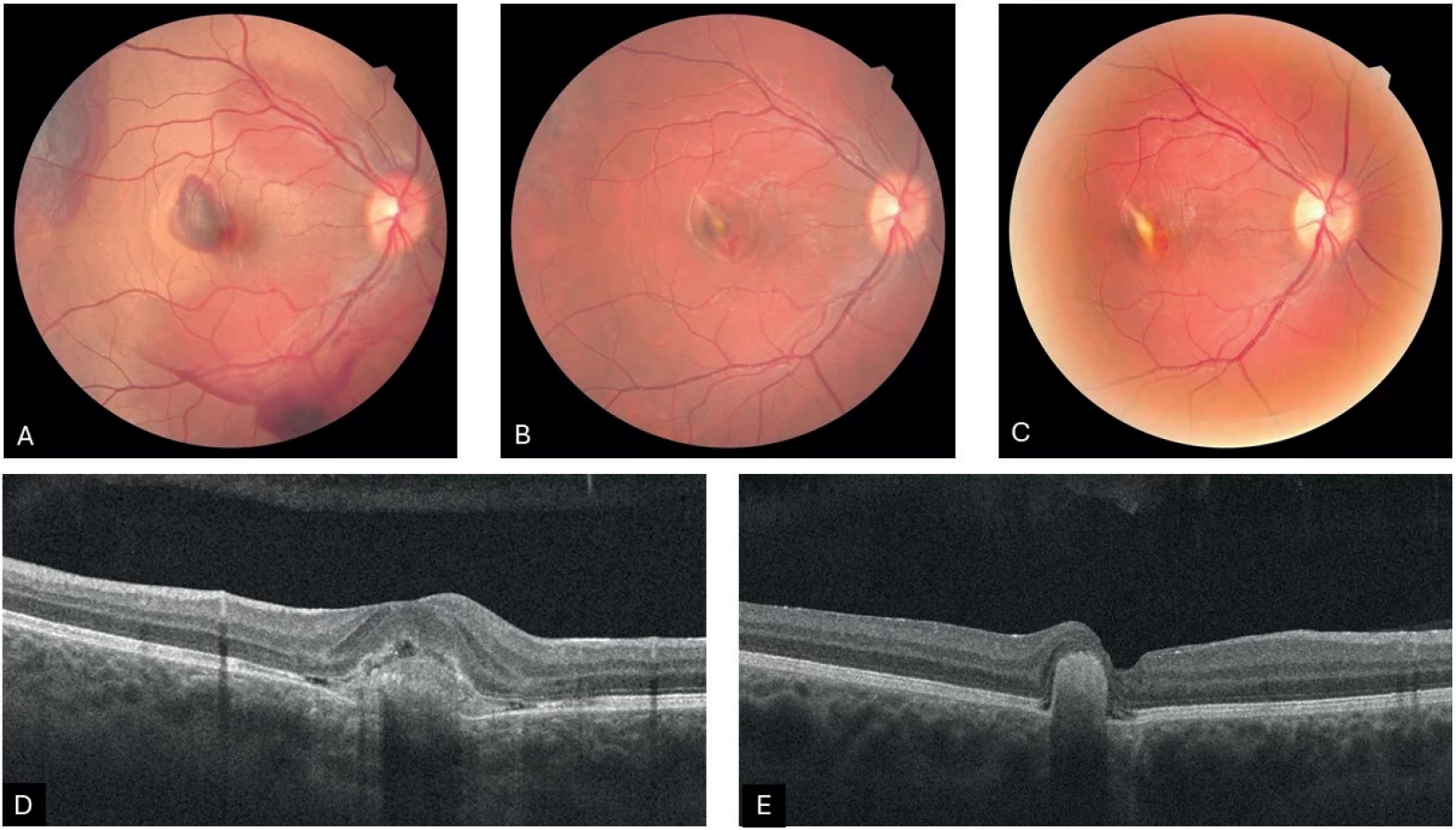
On the basis of the etiological factors, five categories of causes of secondary CNV are defined in the professional literature: post-inflammatory/post-infectious, degenerative/dystrophic, post-traumatic, myopic and neoplastic. In cases where the cause of CNV is impossible to identify, we refer to idiopathic CNV (Figure 1A, B, C) [4].
INDIVIDUAL CATEGORIES OF CNV
Post-inflammatory/post-infectious (Figure 2A, B, C, D, E)
According to recently published studies incorporating the largest cohorts of patients, inflammatory etiology represents the most common cause of choroidal neovascular membrane in children [5–7]. CNV may be manifested in various stages of intraocular inflammation, from active choroiditis or chorioretinitis, through medium-severe uveitis to panuveitis [5]. A very common cause of post-inflammatory CNV is ocular toxoplasma chorioretinitis. Determining the frequency of occurrence of CNV in this pathology is problematic, since the affected patients usually suffer from scotomas as a consequence of chorioretinitis and are frequently unaware of further loss of sight caused by CNV. Other infectious causes of post-inflammatory CNV include ocular toxocariasis, rubeola, syphilis, and in endemic regions a very common cause is ocular histoplasmosis. Significant non-infectious causes include punctate inner choroidopathy, multifocal chorioretinitis, Vogt-Koyanagi-Harada syndrome, serpiginous chorioretinopathy and others [8].
Degenerative/dystrophic (Figure 3A, B, C)
CNV has been documented in a range of retinal dystrophies, such as Best vitelliform macular dystrophy, Stargardt disease and retinitis pigmentosa. This category also covers CNV upon a background of optic nerve drusen or other anomalies of the optic nerve such as coloboma, optic nerve pits and morning glory syndrome. In the case of anomalies of the optic nerve, CNV more commonly has a peripapillary localization [1]. Within the context of pathological myopia, predisposing factors for the occurrence of CNV include RPE atrophy and cracks in the Bruch’s membrane, as a consequence of which CNV is more probable in older patients with degenerative myopia. However, in rare cases it also occurs in the pediatric population.
Post-traumatic (Figure 4A, B, C, D, E)
Most cases of post-traumatic CNV occur during the course of healing of a rupture of the choroidal membrane, though this is not a rule [9]. Risk factors for the development of CNV include proximity of the rupture to the center of the fovea and length of the rupture [10].
Neoplastic (Figure 5A, B, C, D, E)
Within this category, cases have been published of CNV in children upon a background of choroidal osteoma or combined hamartoma of the retina and RPE. Choroidal osteoma is a rare benign intraocular tumor, which typically affects young, otherwise healthy female patients in the first or second decade of life. However, it may also be diagnosed in men, older persons or infants [11,12]. It mostly concerns a unilateral affliction, although bilateral cases have also been described [13,14]. The etiology of choroidal osteoma has not been fully clarified to date. Potential factors under consideration include inflammation, trauma, hormonal changes and disorders of calcium metabolism. Clinically choroidal osteoma is manifested as a yellowish or orange, slightly elevated lesion with well-defined geographical edges. The most common localization is the juxtapapillary or peripapillary region, although it may encroach as far as the macula. The prognosis of this pathology is generally unfavorable, and depends on the presence of complications such as decalcification of the lesion, RPE atrophy, presence of subretinal fluid or secondary CNV. At present no standardized therapeutic protocol is in existence. Treatment is directed towards the management of secondary complications, and includes laser photocoagulation, transpupillary thermotherapy, photodynamic therapy and intravitreal application of anti-VEGF preparations. According to the latest recommendations, intravitreal anti-VEGF therapy is considered a safe and effective method upon the occurrence of secondary CNV upon a background of choroidal osteoma, regardless of the localization of CNV [15,16].
At present intravitreal preparations containing anti-VEGF agents represent the standard therapeutic choice in the management of CNV in pediatric patients. These substances inhibit angiogenesis and reduce vascular permeability, which may lead to stabilization or improvement of visual functions [9]. With the increasing amount of available clinical data confirming the beneficial effect of anti-VEGF therapy on pediatric CNV, the previously preferred methods such as laser photocoagulation and photodynamic therapy are now in decline.

HD-OCT – high-definition optical coherence tomography

HD-OCT – high-definition optical coherence tomography

With reference to the low incidence of this disease, the observations we have to date are based predomi - nantly on a limited number of retrospective studies and case reports, in which no standardized therapeutic protocol has yet been compiled. With reference to the character of the disease and the specifics of the pediatric population, the realization of a prospective randomized controlled trial appears improbable.
MATERIAL AND METHOD
In our cohort of patients we retrospectively analyzed medical records and pictorial documentation of 12 pediatric patients in whom CNV had been diagnosed and treated with an anti-VEGF preparation at our clinic in the period from January 2015 to April 2025. The cohort consisted of 7 male and 5 female patients. All the cases involved unilateral disease; the right eye was affected more commonly (n = 7) in comparison with the left eye (n = 5). The mean age at onset was 11.8 years, with an age range of 3 to 17. The analyzed epidemiological and clinical parameters included: sex, age at time of diagnosis, clinical symptoms, initial best corrected visual acuity (BCVA), final BCVA and the number of applications. Morphological parameters were also evaluated: localization of CNV, etiology of CNV, category of CNV, initial and final central retinal thickness (CRT).
All the patients underwent a comprehensive ophthalmological examination and laboratory blood test. BCVA was examined on a Snellen chart and subsequently converted to a decimal value. CNV was detected by biomicroscopic examination of the ocular fundus and optical coherence tomography (OCT). Fluorescein angiography was used in 7 cases in order to confirm the diagnosis, determine the type of CNV and identify its activity. The subjective complaints in determining the diagnosis included: blurred vision, perception of a greyish deposit and scotoma of the visual field. In two patients no subjective complaints were manifested, and CNV was diagnosed during a routine preventive eye check. The ocular pathologies predisposing the onset of CNV in our cohort include: chorioretinitis (n = 5), punctate inner choroidopathy (n = 1), traumatic choroidal rupture (n = 1), choroidal osteoma (n = 1) and pathological myopia (n = 1). In 3 patients the cause was not clarified and the cases were classified as idiopathic CNV.
HD-OCT – high-definition optical coherence tomography

HD-OCT – high-definition optical coherence tomography
With the aid of OCT scans we compared initial and final CRT. On individual OCT horizontal scans with high resolution we measured retinal thickness in the region of the deposit. Based on the distance of the CNV deposit from the foveal avascular zone, CNV was classified as subfoveal, juxtafoveal (up to 199 µm from the foveola) and extrafoveal (more than 200 µm from the foveola). OCT was also used to monitor the effectiveness of therapy by identifying the presence of intraretinal or subretinal fluid. All the cases represented classic CNV, also known as type 2. According to the OCT examination, average retinal thickness in the location of the deposit before the commencement of therapy was 624 µm (range 451–1050 µm), after treatment 488 µm (range 356–733 µm). Average initial CRT was 325 µm (257–479 µm), final CRT 232 µm. The most common localization of CNV was the subfoveal region, which was affected in 7 patients; in 4 patients CNV was juxtafoveal and in one patient the localization was extrafoveal.
During the course of therapy no standardized protocol was available for the application of anti-VEGF to children. In each patient the number of applications was assessed individually on the basis of the activity of the disease, localization of the lesion and the type of underlying ocular pathology. In 9 cases a fixed dosage of 3 injections at monthly intervals was used, in which activity ceased after the third injection and no further application was indicated. In the case of myopic CNV, due to the extrafoveal localization and only slight deterioration of vision one dose of ranibizumab was applied, which led to the elimination of edema and regression of the thickness of the deposit. The patient remained under observation. In one case of a patient with choroidal osteoma, as a consequence of persistent CNV activity and progressive shortening of the interval between applications a transition to the pharmaceutical preparation aflibercept, in which effectiveness has been recorded in patients not responding to treatment with bevacizumab or ranibizumab, is planned in the forthcoming period [17]. In all cases the standard dose of the drug designated also for adult patients was used – ranibizumab (Lucentis, Novartis, 0.5 mg in 0.05 ml). The application of the pharmaceutical took place under general anesthesia with the aid of a needle with a diameter of 30 gauge (0.3 mm) inserted 3.5 to 4 mm posterior from the limbus. The total average number of applied injections in all patients in the period of observation was 3.4 (range 1 to 10). In three cases of post-inflammatory CNV, in which an infectious etiology was presumed, the patients were treated with general antibiotic and corticosteroid therapy before the application of the anti-VEGF treatment.
Between the individual applications the patients underwent regular outpatient monitoring examinations, which incorporated assessment of BCVA, examination on a slit lamp, biomicroscopic examination of the ocular fundus, and if necessary photography of the ocular fundus and OCT examination. The average observation period was 35 months, with a range of 5 to 97 months.
RESULTS
Mean initial BCVA was 0.277 decimal (logMAR 0.56), with a range of 0.014 to 1.0 decimal. After the conclusion of therapy, mean final BCVA attained a value of 0.65 decimal (logMAR 0.19), within the range of 0.133 to 1.0 decimal. Acquired visual acuity (VA) was on average 0.38 decimal. A deterioration of VA was not recorded in any of the patients. Mean reduction of CRT was 94.9 µm. In all cases a positive functional or anatomical effect was observed. Throughout the entire observation period no adverse ocular or systemic effect was recorded in association with the application of ranibizumab.
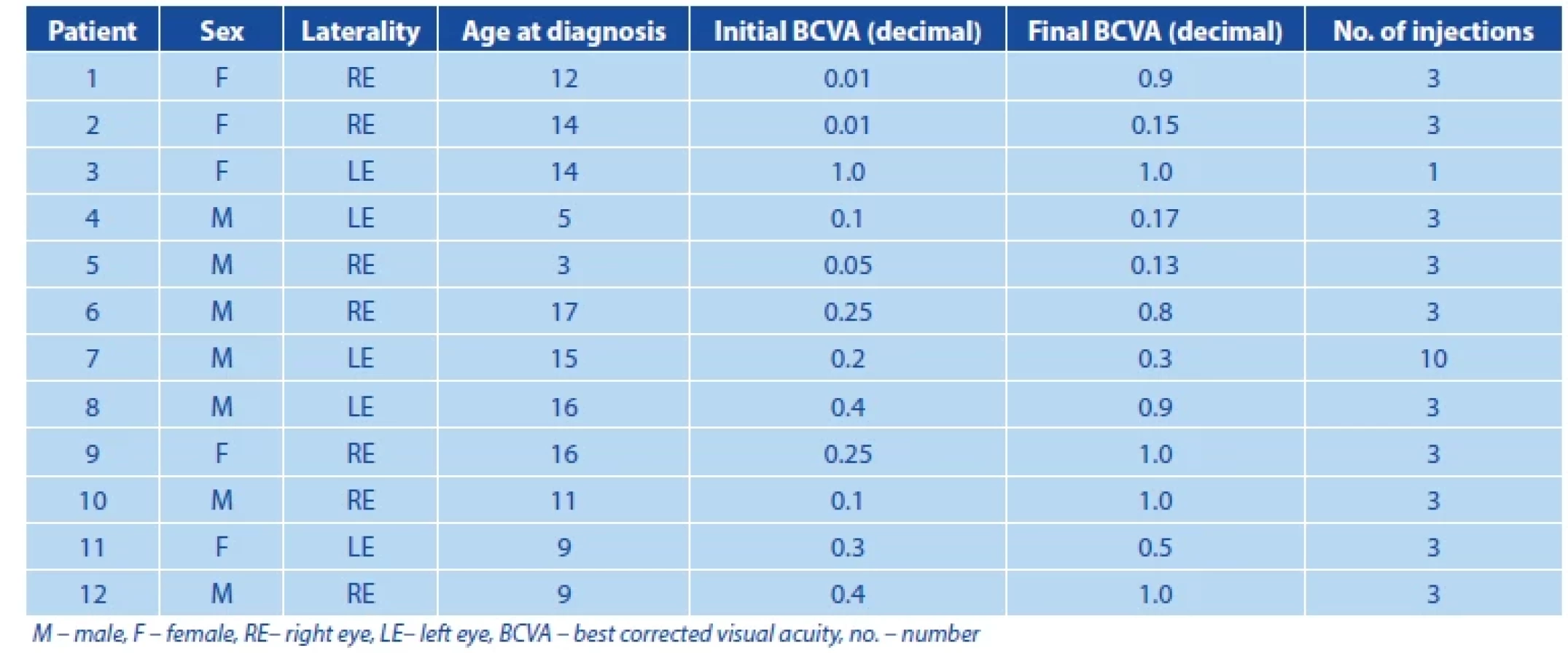
More detailed characteristics of the individual cases are described in the tables. Table 1 summarizes the following epidemiological and clinical data: sex of patient, age at time of diagnosis, initial and final BCVA, number of intravitreal injections. Table 2 presents morphological data: localization, etiology and category of CNV, initial and final CRT.
DISCUSSION
Although choroidal CNV is considered a rare disease within the pediatric population, from the perspective of the number of years it is experienced by the patient its impact is significant. To date only a small number of retrospective studies have been published describing the incidence of CNV in children. The first and so far only population data on the incidence of CNV were published in a study by Moosajee et al. from the United Kingdom relating to children aged 16 years or younger, with an annual incidence of 0.21 per 100 000 [7]. Knowledge of CNV in adults cannot be directly extrapolated to the pediatric population, since the pathogenesis and clinical course of CNV in children differs markedly from those in adults. Unlike the development of CNV in the older population, where in most cases the cause is exudative ARMD, in children a different underlying ocular pathology is often present.
As regards the etiology of CNV in children, a variety of most common causes are stated in the professional literature. According to the publication by the authors Moosajee, Rishi et al., the most common cause is inflammatory pathology, whereas in the studies by the authors Rego-Lorca, Padhi et al. the most common cause is stated as Best disease [5–7,18,19]. In our cohort of patients the most common etiology was post-inflammatory and post-infectious, which occurred in 50% of cases, followed by idiopathic etiology. An idiopathic cause was represented in 25% of our cohort, which corresponds approximately with the proportion of CNV with idiopathic origin presented in other studies [2,20,21].
In general it is possible to state that the most com - mon causes of pediatric CNV according to the available data include chorioretinitis and Best disease. However, in our cohort we did not encounter a diagnosis of hereditary retinal dystrophy, which may be a consequence of the limited number of patients. The average age upon determination of the diagnosis of pediatric CNV is consistent across the majority of studies, and is within the range of 11 to 12 years.

In accordance with the data published to date, in our cohort of patients we recorded a markedly higher incidence of subfoveal form of CNV in comparison with juxtafoveal and extrafoveal forms [1,5,6,19,21]. The higher frequency of the classic form of CNV in comparison with occult or mixed forms also corresponds with the data presented in the literature [19]. These findings, like the lower number of applications in comparison with the treatment of CNV in the adult population, are probably linked to the better functional integrity of the RPE and the absence of chronic degenerative changes of this layer in pediatric patients [21,22].
The therapeutic approach in pediatric patients with CNV is individual, and depends on the activity, localization and presence of other predisposing pathologies. It may also differ according to the experiences of the center in question. In a study conducted by Zhang et al. it is stated that an effective therapy is 1 initial injection of anti-VEGF preparation followed by a pro re nata regimen [6]. In our cohort a fixed application schema was used on 9 patients, consisting of 3 injections at monthly intervals. In the case of myopic extrafoveal CNV an individual dose was administered with complete elimination of activity of the deposit, and in the case of CNV associated with choroidal osteoma, due to persistent activity of CNV after the fixed loading phase, this was followed by therapy in a pro re nata regimen.
Mean BCVA upon determination of the diagnosis in our cohort was logMAR 0.56, which is a slightly higher value than stated in other studies. For example, Rishi et al. state logMAR 1.02 [5], Ranjan et al. mean logMAR 0.8 [23] and Rego-Lorca et al. logMAR 0.57 [18]. By contrast Finn et al. state mean BCVA at logMAR 0.53 upon determination of the diagnosis [11]. In most of the published studies an improvement of VA was recorded during the course of observation. Rishi et al. recorded a final improvement to logMAR 0.87, Ranjan et al. state an improvement from logMAR 0.8 to 0.4, while Finn et al. attained an average BCVA of 0.37. In our cohort there was a significant improvement of BCVA from a mean logMAR of 0.56 to 0.19. A comparison of the results from different studies shows considerable variability in the clinical manifestations and prognosis in pediatric patients with CNV. This variability is probably caused by the differences in the etiology of origin of CNV and subsequent pathophysiological mechanisms that influence final VA and the activity of the pathology.
An interesting finding is the distribution of frequency of cases in our cohort during the course of the observation period. In the years 2015 and 2016 no treatment with injections of anti-VEGF for CNV was indicated at our clinic. We recorded the largest number of diagnosed cases and indications for therapy in 2024 and in January and February of this year. The increase in the incidence in the most recent years is probably due to better diagnostic possibilities and increased awareness among professionals in the field concerning the incidence and options for treatment of CNV in children. Some studies indicate that this may also represent an increased incidence of predisposing pathologies within this age group [25].
No adverse ocular symptoms were recorded during the observation of our patients. However, it is necessary to note that long-term data on the metabolism of anti-VEGF molecules in children is unavailable to date. VEGF plays a crucial role in normal angiogenesis, regulation of permeability of vessels and maintaining the functions of the blood-brain and blood-retinal barriers. It is not yet clear as to how serum levels of anti-VEGF influence the child brain [24]. As a result it is essential to carefully monitor the long-term effects of inhibition of these functions in the pediatric population.
With reference to the rare nature of pediatric CNV, it is not possible to expect the realization of large randomized controlled trials. As a result it is probable that intravitreal anti-VEGF therapy shall continued to be considered an off-label indication [20].
CONCLUSION
CNV in children represents a very rare pathology, a consequence of which is the limited amount of published data, and no specific therapeutic protocol for the treatment of this disease in the pediatric population exists to date. However, without adequate treatment CNV may constitute a significant threat to sight. In our cohort of patients, as well as in the studies published to date, therapy of pediatric CNV with the aid of an anti-VEGF preparation appears to be a safe and effective method of treating this diagnosis in children.
Nevertheless, as yet there are no available data concerning the long-term side effects or metabolism of anti-VEGF molecules in children, which may differ from the data obtained in the adult population. For this reason it is important to continue to focus systematically on this subject, and to publish the obtained clinical data.
Zdroje
- Rego-Lorca D, Català-Mora J, López-de-Eguileta A, Díaz-Cascajosa J. Choroidal neovascularization in children: etiology, clinical characteristics and treatment outcomes. Arch Soc Esp Oftalmol (Engl Ed). 2024 Dec;99(12):534-539.
- Cohen SY, Laroche A, Leguen Y, Soubrane G, Coscas GJ. Etiology of choroidal neovascularization in young patients. Ophthalmology. 1996 Aug;103(8):1241-1244.
- Carneiro AM, Silva RM, Veludo MJ, et al. Ranibizumab treatment for choroidal neovascularization from causes other than age-related macular degeneration and pathological myopia. Ophthalmologica. 2011;225(2):81-88.
- Goshorn EB, Hoover DL, Eller AW, Friberg TR, Jarrett WH, Sorr EM. Subretinal Neovascularization in Children and Adolescents. Journal of Pediatric Ophthalmology & Strabismus. 1995 May;32(3):178782.
- Rishi P, Bharat RPK, Rishi E, et al. Choroidal neovascularization in 111 eyes of children and adolescents. Int Ophthalmol. 2022 Jan;42(1):157-166.
- Zhang T, Wang Y, Yan W, et al. Choroidal Neovascularization in Pediatric Patients: Analysis of Etiologic Factors, Clinical Characteristics and Treatment Outcomes. Front Med (Lausanne). 2021;8 : 735805.
- Moosajee M, Abbouda A, Foot B, Bunce C, Moore AT, Acheson J. Active surveillance of choroidal neovascularisation in children: incidence, aetiology and management findings from a national study in the UK. Br J Ophthalmol. 2018 Apr;102(4):438-443.
- Niederer R, Bar A, Al-Ani H, et al. Management of inflammatory choroidal neovascular membranes. Expert Review of Ophthalmology. 2021 Jan 2;16(1):47-60.
- Rishi P, Gupta A, Rishi E, Shah BJ. Choroidal neovascularization in 36 eyes of children and adolescents. Eye (Lond). 2013 Oct;27(10):1158-1168.
- Secrétan M, Sickenberg M, Zografos L, Piguet B. Morphometric characteristics of traumatic choroidal ruptures associated with neovascularization. Retina. 1998;18(1):62-666.
- Choroidal osteoma in old age (an unexpectedly difficult diagnosis). Acta Ophthalmol. 2018 Dec;96(S261):67-68.
- Aksoy Y, Çakir Y, Sevinçli S, Sönmez M, Ayata A. Choroidal osteoma in a preterm infant. Ind J Ophthalmol. 2018 Apr;66(4):583-585.
- Fine HF, Ferrara DC, Ho IV, Takahashi B, Yannuzzi LA. Bilateral choroidal osteomas with polypoidal choroidal vasculopathy. Retin Cases Brief Rep. 2008;2(1):15-17.
- Huang YM, Zhang L, Liang J, Yuan RD. Bilateral choroidal osteoma with unilateral polypoidal choroidal vasculopathy treated with conbercept. Int J Ophthalmol. 2020;13(6):1009-1012.
- Gómez PD, Català-Mora J, López-de-Eguileta A, Díaz-Cascajosa J. Bilateral choroidal osteoma: long-term follow-up of secondary choroidal neovascularization in a child using antiangiogenic therapy. Japoos. 2024;Vol 28: Issue 2103869. doi:10.1016/j.jaapos.2024.103869
- Zhang L, Ran QB, Lei CY, Zhang MX. Clinical features and therapeutic management of choroidal osteoma: A systematic review. Survey of Ophthalmology. 2023 Nov 1;68(6):1084-1092.
- Saitta A, Nicolai M, Neri P, Reibaldi M, Giovannini A, Mariotti C. Rescue therapy with intravitreal aflibercept for choroidal neovascularization secondary to choroidal osteoma non-responder to intravitreal bevacizumab and ranibizumab. Int Ophthalmol. 2015 Jun;35(3):441-444.
- Rego-Lorca D, Català-Mora J, López-de-Eguileta A, Díaz-Cascajosa J. Choroidal neovascularization in children: etiology, clinical characteristics and treatment outcomes. Archivos de la Sociedad Española de Oftalmología (English Edition). 2024 Dec;99(12):534-539.
- Padhi TR, Anderson BJ, Abbey AM, et al. Choroidal neovascular membrane in paediatric patients: clinical characteristics and outcomes. Br J Ophthalmol. 2018 Sep;102(9):1232-1237.
- Barth T, Zeman F, Helbig H, Oberacher-Velten I. Etiology and treatment of choroidal neovascularization in pediatric patients. Eur J Ophthalmol. 2016 Oct;26(5):388-393.
- Kozak I, Mansour A, Diaz RI, et al. Outcomes of treatment of pediatric choroidal neovascularization with intravitreal antiangiogenic agents: the results of the KKESH International Collaborative Retina Study Group. Retina. 2014 Oct;34(10):2044-2052.
- Kim R, Kim YC. Intravitreal ranibizumab injection for idiopathic choroidal neovascularization in children. Semin Ophthalmol. 2014 May;29(3):178-181.
- Ranjan R, Salian R, Verghese S, et al. Pediatric choroidal neovascularization: Etiology and treatment outcomes with anti-vascular endothelial growth factors. Eur J Ophthalmol. 2022 Jul;32(4):2355-2367.
- Sivaprasad S, Moore AT. Choroidal neovascularisation in children. Br J Ophthalmol. 2008 Apr;92(4):451-454.
- Finn AP, Fujino D, Lum F, Rao P. Etiology, Treatment Patterns, and Outcomes for Choroidal Neovascularization in the Pediatric Population: An Intelligent Research in Sight (IRIS®) Registry Study. Ophthalmology Retina. 2022 Feb 1;6(2):130-138.
Štítky
OftalmológiaČlánok vyšiel v časopise
Česká a slovenská oftalmologie

2025 Číslo Ahead of Print
- Pomocné látky v roztoku latanoprostu bez konzervačních látek vyvolávají zánětlivou odpověď a cytotoxicitu u imortalizovaných lidských HCE-2 epitelových buněk rohovky
- Konzervační látka polyquaternium-1 zvyšuje cytotoxicitu a zánět spojený s NF-kappaB u epitelových buněk lidské rohovky
- Dlouhodobé výsledky lokální léčby cyklosporinem A u těžkého syndromu suchého oka s 10letou dobou sledování
- Syndrom suchého oka
- Cyklosporin A v léčbě suchého oka − systematický přehled a metaanalýza
Najčítanejšie v tomto čísle
- Clinical Outcomes of Preserflo MicroShunt versus Trabeculectomy: A Retrospective 6-Month Study
- Choroidal Neovascular Membrane in Pediatric Patients: Long-Term Outcomes of Anti-VEGF Therapy
- Utility of in Vivo Corneal Confocal Microscopy in Atypical MEN2B Findings. A Case Report
- Hyperreflective Outer Nuclear Layer as a Biomarker of Early Stargardt Disease. A Case Report