
Improvement of Visual Field Defects after Neuroembolization Treatment of Intracranial Aneurysms. Case Reports
Authors:
Nora Majtánová 1,2
![]() ; Petr Kolář 1,2
; Petr Kolář 1,2
![]() ; Petra Krišková 1
; Petra Krišková 1
![]() ; Petra Kéri 1
; Petra Kéri 1
![]() ; Tibor Balazs 3; Dalibor Cholevík 1,2; Veronika Kurilová 1
; Tibor Balazs 3; Dalibor Cholevík 1,2; Veronika Kurilová 1
Authors place of work:
Department of Ophthalmology, Slovak Medical University and University Hospital, Bratislava, Slovakia
1; Faculty of Medicine, Slovak Medical University, Bratislava, Slovakia
2; CINRE Center for Interventional Neuroradiology and Endovascular Treatment, Bratislava, Slovakia
3
Published in the journal:
Čes. a slov. Oftal., 80, 2024, No. 1, p. 42-51
Category:
Kazuistika
doi:
https://doi.org/10.31348/2024/8
Summary
Purpose: Intracranial aneurysms and their hemorrhagic and thromboembolic complications represent a serious nosological unit that significantly endangers those afflicted. They are mostly asymptomatic until rupture occurs. In two case reports, we present our observations of young patients with impaired vision and headaches, in whom we found the presence of intracranial aneurysms.
Observations: Presentation of two case reports of patients who came to our department with impaired vision and headaches. The patients underwent a complete eye examination at our center, including a visual field examination. Based on the results of the examination, they were referred for
an imaging examination of the brain, which revealed the presence of intracranial aneurysms. The patients were subsequently sent to the interventional neuroradiology center, where they underwent a noninvasive endovascular neuroembolization procedure with flow diverter implantation. We continued to monitor the patients after the procedure and document the examination results up to 1 year after the procedure.
Conclusions and significance: Thanks to the fast detection, diagnosis, and management of both patients, we prevented the occurrence of aneurysm rupture, thus a life-threatening complication. After endovascular procedures with flow diverter implantation, we observed a significant improvement in visual acuity as well as perimetric findings in both patients. When intracranial aneurysms are found within a week of the onset of eye symptoms and treated within three months, defects in the visual fields improved in our two patients within 6–12 months, and in one of the two patients the defects almost completely disappeared.
Introduction
The most common manifestation of intracranial aneurysms is subarachnoid hemorrhage [1]. The majority of aneurysms remain asymptomatic up to the point of rupture. Symptoms are present prior to rupture in only 10% of carriers, triggered especially by pressure on brain structures, as well as in the tumor growth process [2]. The presence of a giant aneurysm is therefore frequently confirmed by differential diagnosis of a brain tumor [3]. The risk of rupture is greater in the case of symptomatic aneurysms than in asymptomatic, and as a consequence, treatment should always be considered not only in order to alleviate pressure on brain structures, but also to prevent the occurrence of rupture [4]. With regard to the close localization of the circle of Willis with structures of the visual pathway, some aneurysms may grow close to the optic nerve, the optic chiasm, the optic tract or the optic radiation, which generates pressure on these anatomical structures and varying degrees of visual deficit [5,6]. Disorders of vision as a symptom of intracranial aneurysms are described by authors only in the case of larger to giant aneurysms (15–24 mm, 25 mm and larger) [5,7]. Loss of sight as a consequence of ruptured intracranial aneurysms is explained in most cases by Terson’s syndrome [8], which most often occurs as a consequence of subarachnoid hemorrhage following the rupture of an aneurysm of the anterior communicating artery. The finding is typically bilateral and is manifested in multiple retinal hemorrhage. In this case it is always difficult to assess whether the deterioration of visual acuity is predominantly due to a central cause or as a result of intraocular hemorrhage [9].
A common manifestation of an unruptured intracranial aneurysm is headache, which is present in approximately one third of cases [10]. Pain in the head may be manifested as new and acute, but also chronic and non-specific. With regard to the fact that chronic headache is a frequent manifestation of other pathologies, the possibility of presence of an intracranial aneurysm may not always be considered by the doctor. Other symptoms may include relative afferent pupillary defect, convulsions and difficulties performing regular daily activities. Oculomotor disorders also frequently occur [9].
Intracranial aneurysms, as well as various other intracranial expansions, may lead to a range of defects in the visual field. Furthermore, defects in the visual field may not be identical upon their repeated examination in the same patient. The mechanism of onset of defects in the visual field may be ischemia, compression or direct hemorrhage into the optic nerve or chiasm. Direct infiltration into the optic nerve or direct damage thereto by an aneurysm is extremely rare [11]. Their character may provide an indication of the localization of the pathology. We register different changes in the visual field in the case of pathology in the orbit, chiasm, and retrochiasmally. Compression or ischemia of the chiasm may be caused by an aneurysm of the anterior communicating artery or the internal carotid artery. Retrochiasmally, vascular causes, e.g. aneurysms, appear more commonly in adults, in contrast with children, in whom tumors are a more frequent cause [12]. In Table 1 we describe the most common localizations of aneurysms encroaching upon the visual pathway according to the available literature, with the pressure point and the most commonly manifested changes in the visual field. We also illustrate this data schematically in Fig. 1, where we visualize the relationship of the visual pathway with the intracranial circle of Willis, potential localizations of aneurysms and the pressure points they may cause, together with the corresponding defects in the visual field if pressure is sufficiently manifested.
Two approaches are applied for the treatment of intracranial hemorrhages – surgical, directly during open craniotomy – most often clipping, or less invasive, endovascular coiling with the aid of detachable microspirals and/or flow diverters. Schuss et al. presented an inferior success rate with the improvement of defects in the visual field upon endovascular treatment (38%) in comparison with the surgical procedure, clipping (75%) [15]. In contrast with this finding, Lu et al. [16] compared impairment of vision and defects in the visual field after clipping and endovascular treatment of aneurysms of the ophthalmic artery in favor of endovascular treatment (2.4% versus 16.1%). Date et al. [5] describe an improvement in the visual field in 63.6% of patients with larger to giant intracranial aneurysms following a clipping or ligation operation, in which these patients were operated on within three months of the detection of visual disorders. In 36.4% of cases the patients were operated on after more than three months, upon which no improvement in the visual field was achieved. The success of clipping was also confirmed by a study conducted by de Oliveira et al. [13], in which complete disappearance of the defects in the visual field was achieved postoperatively in 46.6% of cases, and an improvement was achieved in the same percentage of patients with an aneurysm compressing the anterior part of the visual pathway. Vargas et al. [14] describe 19 giant intracranial aneurysms with impaired vision treated by endovascular embolization using detachable balloons, and with the use of Guglielmo detachable microspirals. The study points to promising results and a low rate of complications in the group with the use of microspirals, and also explains when it may be an advantage to use the balloon technique.
On the other hand, endovascular treatment of aneurysms may also cause impairment of vision and the visual field – Ferrel et al. [17] describe a delayed finding in the visual field in two patients. Delayed visual deficit following the successful endovascular treatment of a giant paraophthalmic aneurysm in six patients is described by Raymond et al. [18], who analyze the individual types of materials of the microspirals used.
The aim of this article is to familiarize readers with the potential manifestations of intracranial aneurysms during a perimetric examination, which may first be encountered by an ophthalmologist, who can then report suspicion of this diagnosis. Knowledge of this issue and the therapeutic options enables timely diagnosis and treatment before rupture, thereby averting permanent changes in the visual field. In the following case reports we present two young patients in whom we determined the presence of intracranial aneurysms. Thanks to fast management a timely surgical intervention was performed, by which we averted the occurrence of rupture and a life-threatening condition.
Table 1. The most frequent localizations of the aneurysms affecting the visual pathway, with the place of compression, and the most frequently listed visual field defects according to the available literature
|
Localizations of the aneurysms |
Place of compression (if listed), event. probable place of compression* |
Author of the publication |
Most frequently listed visual field defect |
|
Arteria communicans anterior |
chiasma opticum |
Oliveira [13] |
bitemporal hemianopsia |
|
n. opticus, fibers from nasal retina* |
Oliveira [13] |
unilateral temporal hemianopsia |
|
|
Park [3] |
|||
|
Vargas [14] |
|||
|
Arteria carotis internaintracavernous / paraclinoidal |
nervus opticus* |
Vargas [14] |
homolateral unilateral quadrantopsia to hemianopsia |
|
Oliveira [13] |
|||
|
Arteria carotis internasupraclinoidal |
chiasma opticum, nasal fibers* |
Vargas [14] |
bitemporal quadrantopsia or hemianopsia |
|
Arteria carotis internabifurcation |
tractus opticus |
Oliveira [13] |
contralateral homonymous hemianopsia |
|
Arteria cerebri media proximal segment (occasionally, huge aneurysm) |
tractus opticus |
Oliveira [13] |
contralateral homonymous hemianopsia |
|
Arteria communicans posterior (occasionally, huge aneurysm) |
tractus opticus* |
Vargas [14] |
contralateral homonymous hemianopsia |
|
Arteria cerebri posterior |
radiatio optica* |
Vargas [14] |
bilateral quadrantopsia |


CASE REPORT 1
In November 2021 a 29-year-old patient came to our center via the central admissions department. He stated oedema around the right eye persisting for one day, with impaired vision in the right eye, and headache. He had not previously undergone any eye surgery or suffered ocular or head trauma. The patient was not being treated for any general pathology or taking any medications.
The patient’s best corrected visual acuity (BCVA) was 20/40 in both eyes. Intraocular pressure was within the referential range. At an ophthalmoscopic examination, drooping of the upper right eyelid was observed, with no pathological finding on the remainder of the anterior segment in both eyes. On the ocular fundus there was bilateral presence of a pale optic nerve head with cup to disc ratio of 0.5 and nasalization of the central retinal vessel trunk. The macula, blood vessels and retina were without pathological findings bilaterally. On optical coherence tomography (OCT) of the optic nerve head, reduced thickness of the retinal nerve fibers was determined (Fig. 2, first column from left), and pathological values were recorded in all quadrants in the ganglion cell complex (Fig. 2, central column). The patient also underwent a perimetric examination by an above-threshold testing strategy within the range of 60 degrees of the visual field, in which numerous scotomas were identified in both eyes (Fig. 2, last column from left). We subsequently added a 24-2 threshold testing strategy with a finding of bitemporal hemianopsia, with overlapping across the vertical line. The patient was urgently referred for CT of the brain with a contrast substance.
The CT examination detected a finding of multiple fusiform aneurysms: on the level of the internal carotid artery (ACI) / middle cerebral artery (ACM) on the left side (C7/M1) fusiform enlargement of the vascular lumen 18 x 10 mm with calcification of the vascular walls centrally. In the direction towards the periphery on the level close before the bifurcation (M2) of the ACM on the left side there was a finding of fusiform lumen enlargement of 7.8 x 6.8 mm. Ectatic enlargement was present also on the level of the initial part of M1 ACM on the left side, in combination with minor calcification of the vascular walls. Similar fusiform dilation of the lumen was also found in the course of the posterior cerebral artery (ACP) on the left side, section P3, approx. 10 x 7 mm. The anterior inferior cerebellar artery on the left side was irregularly ectatically enlarged in comparison with the contralateral side. No significant stenoses were found in the course of the displayed blood vessels.
Based on a CT examination of the brain, the patient was admitted to the neurological department, where magnetic resonance (MR) of the brain with a contrast substance was performed, focusing on the orbits and the visual pathway. The MR scan described a finding of multiple fusiform aneurysms in the blood vessels of the circle of Willis, in which the largest aneurysm was in the place of bifurcation of the ACI on the left side, crossing over to the M1 section of the ACM on the left side. The aneurysm was compressing the optic tract on the left side after the gap from the chiasm, with dorsomedial deviation of the optic tract. The radiologist indicated the presence of this aneurysm as the cause of the complaints and recommended an urgent consultation with an interventional radiologist.
The patient was subsequently transferred from the surgery department to the center for interventional neuroradiology and endovascular treatment (CINRE). On rotation angiography with 3D reconstruction, a finding of extensive intracranial fusiform bifurcation aneurysms was verified: in the distal carotid siphon of the ACI on the left side C7/A1 (22 mm), in the branching of M1 and bifurcation of the ACM on the left side (11 x 7 mm), P2-P3 ACP on left (13 mm) (Fig. 3, upper row). Sequential emergent neuroembolization treatment (NEMB) of the swellings by flow diversion was indicated, with controlled thrombolysis in long-term dual anti-platelet therapy (DAPT).
NEMB of the swelling of P2/P3 ACP on the left side was performed under general anesthesia, by transfemoral approach from the right. After fourteen days the patient underwent a further NEMB of a swelling of C7/M1 ACM on the left side (Fig. 3, second row). The aim of implanting of a flow diverter device (FDD) in this patient was not to immediately eliminate the swellings, but to reduce them by redirecting the flow. In the opposite case, sudden stroke may have occurred. Fig. 3, bottom row illustrates the gradual shrivelling of both aneurysms over time on digital subtraction angiography (DSA). The bifurcation swelling of the ACM 1.sin. remained temporarily under observation without the need for intervention.
Two months after the interventions, the patient stated a subjective pronounced improvement in the opening of the right eye and visual acuity. His BCVA in the right eye improved to 20/25, in the left eye there was a progression to 20/63. The objective drooping of the upper right eyelid was now less pronounced but still persisted, the other ophthalmoscopic finding was without any changes. We administered topical (brimonidine drops 2x per day in both eyes) and general neuroprotective treatment (citicoline 250 mg, oral solution, 3x per day) to the patient.
Both BCVA and the ophthalmoscopic finding remained stable 12 months after the interventions, while there was a progressive improvement of the finding on perimetry after six and twelve months. A comparison of the finding on 24-2 perimetry upon admittance and at 6 and 12 months after the endovascular procedures is illustrated in Fig. 4.
On OCT the layer of the ganglion cell complex remained pathological in all quadrants in both eyes twelve months after the interventions. At the same time, during the course of the year there was a diminution of the retinal nerve fiber layer on the optic nerve head OCT. The patient remained under the observation of a neurologist, an interventional radiologist and an ophthalmologist.

FD – Flow Diverter

CASE REPORT 2
A 28-year-old patient referred to our center in May 2021 with severe headaches and impaired vision in the left eye persisting for 3 days. He had been observed by a neurologist due to headaches over the course of several years. The patient had no history of eye surgery or ocular trauma. He was not being treated for any general pathology and was not taking any medications. BCVA in the right eye was 20/20, and in the left eye on the level of counting fingers in front of the eye. Intraocular pressure was 20/24 mmHg. On an ophthalmoscopic examination the anterior segment was without any pathological finding, on the ocular fundus there was a temporally pale optic nerve head, with cup to disc ratio of 0.2 in both eyes. The blood vessels, retina and macula were without pathological findings bilaterally. The finding was physiological on OCT of the macula, on OCT of the optic nerve head in the right eye the T quadrant was borderline, in the left eye without reduction in the retinal nerve fiber layer (Fig. 5, first column from left). OCT showed a pronounced reduction of the ganglion cell complex, with all the quadrants pathological in the left eye (Fig. 5, second column).
We supplemented a 24-2 examination of the patient’s visual field, where there was the temporal half visual field defect in the right eye and almost entire visual field defect in the left eye. On perimetry within a range of 60 degrees, due to poor psychological coping with the situation of sudden deterioration of vision, the patient ceased to co-operate and refused to undergo further examination.
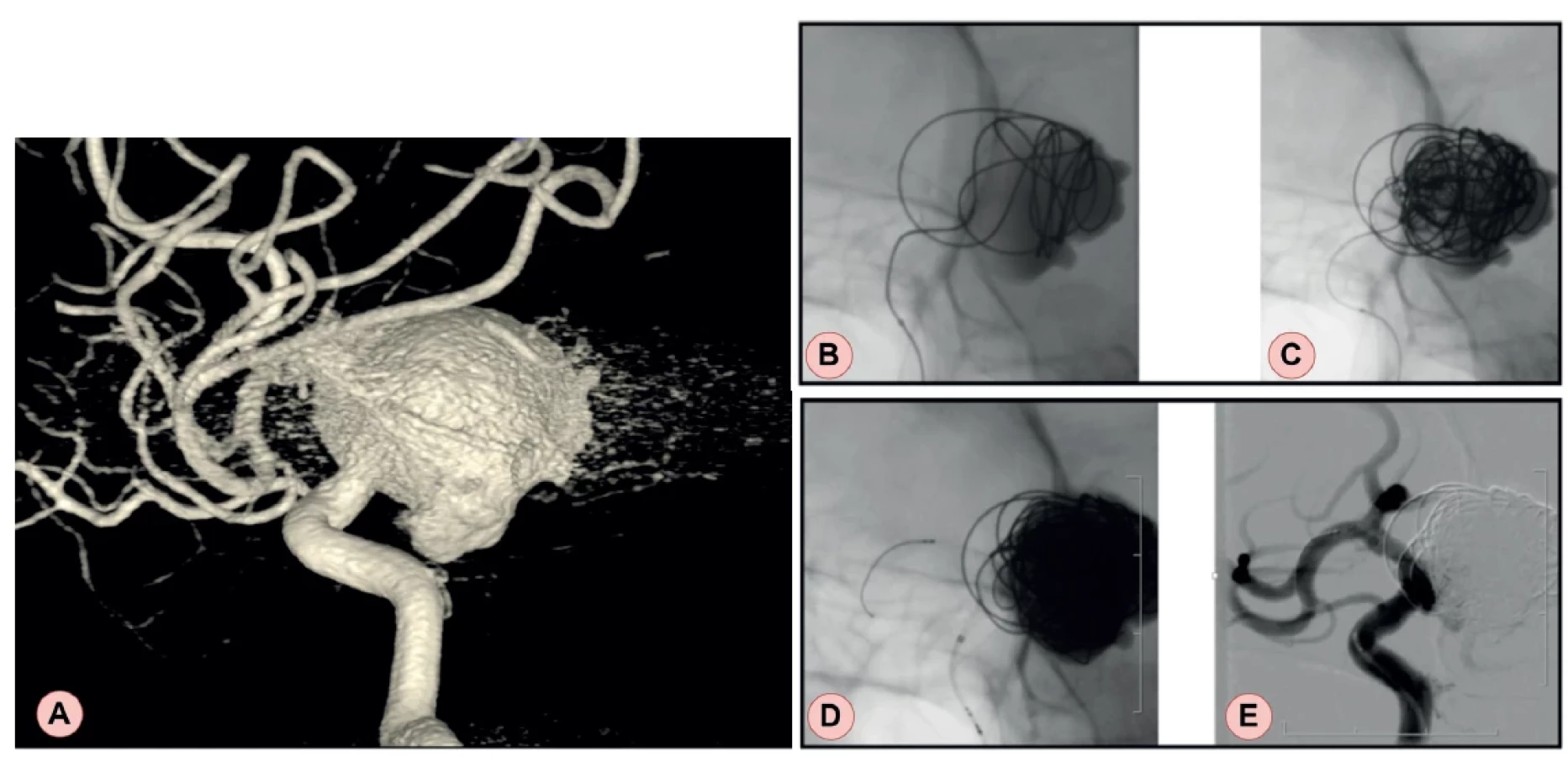
We referred the patient for magnetic resonance of the brain with a contrast substance, in which the presence of a giant aneurysm (27 mm) was determined, emerging from the terminal section of the internal carotid artery on the left side, with a slightly infiltrating wall, compressing the optic chiasm and infundibulum, which is deviated to the right. The patient was urgently sent to the center for interventional neuroradiology and endovascular treatment (CINRE). On rotation angiography with 3D reconstruction, a finding of a gigantic aneurysm of the C6/7 segments of the ACI on the left side was confirmed (Fig. 6, A). The patient was indicated for NEMB. The procedure was performed under general anesthesia, commenced with a transfemoral approach from the right, in which the aneurysm of C6/7 ACI on the left side was cannulated using a microcatheter. Subsequently 17 detachable microspirals were implanted into the cavity of the aneurysm for the purpose of inducing thrombolysis of the aneurysmal sac (Fig. 6 B, C). At a DSA control examination a large part of the aneurysm had been thrombolyzed. At the same time, the cervix of the aneurysm was treated with the implantation of two FDDs for the purpose of redirecting the flow into the mother ACI artery, and optimal apposition of the FDDs was attained by a Commanechi supplementary dilation device. At a control DSA after 2 months the aneurysm persisted completely obliterated, without reperfusion of the sac and without severe contraction of the FDDs (Fig. 6 D, E, bottom row).
One week after the operation the patient reported to our center. His BCVA and ophthalmoscopic finding were unchanged. Due to repeatedly measured higher values of intraocular pressure and atrophy of the optic nerve according to OCT, we administered local anti-glaucomatous therapy (carteolol drops 1x per day early morning) in both eyes, and general neuroprotection (citicoline 250 mg, oral solution, 3x per day). Due to headache following application of the therapy, carteolol was replaced with brimonidine drops 2x per day early morning in both eyes. The patient reported for a follow-up examination three months after surgery, at which his BCVA in both eyes was now 20/20. At further follow-ups, BCVA, the ophthalmoscopic finding and OCT of the optic nerve papilla and ganglion cell complex remained unchanged up to twelve months after surgery, during which time there was a pronounced improvement of the finding on perimetry six months after surgery. A comparison of the patient’s finding on perimetry upon admittance and six months after the endovascular procedure is presented in Fig. 7.


DISCUSSION
At our clinic we examined two patients who reported with acute impairment of vision and headache. On the basis of these subjective complaints, we supplemented perimetry, which confirmed defects in the visual field. Through an examination of the visual field, we predicated the potential central cause of the complaints in the patients and referred them for urgent neuro-imaging examinations, which are an integral component of the diagnosis of intracranial aneurysms. In recent years imaging methods of aneurysms have been considerably expanded thanks to advanced technology and the availability of MR angiography (MRA), CT angiography (CTA) and digital subtraction angiography (DSA). Each imaging modality has its advantages and disadvantages [19]. CTA is a frequently used modality for imaging and screening of intracranial aneurysms. On the basis of a meta-analysis, sensitivity of the CTA is within a range from 53% for 2 mm aneurysms to 95% for 7 mm aneurysms. Overall total specificity is 98.9% [20]. CTA is very useful for identifying calcification of the walls and thrombosis, which may have a significant influence in the management of treatment [21]. However, it is limited by artefacts of bones and metals (stents, clips, …), which limits its effectiveness in noninvasive monitoring of patients after treatment. Exposure to radiation is a further negative factor in long-term observation [22]. MRA is another important imaging method for intracranial aneurysms, though its sensitivity in detecting small aneurysms (< 3 mm) is lower. According to the authors, the sensitivity of examination is described at 95%, and specificity 89%. False positive and false negative aneurysms have been displayed mainly in the region of the cranial base and the middle cerebral artery [23]. The advantage of MR and CT is that they provide information about the brain tissue and adjacent structures in relation to the aneurysm. Data exist which support the use of MRA in long-term observation of the patient [24]. DSA remains the gold standard of imaging methods for intracranial aneurysms. With the aid of techniques such as 3D rotation angiography it is possible to identify small aneurysms. Another advantage is morphological assessment of aneurysms. However, this examination has a small risk of onset of ischemic vascular stroke, dissection, hemorrhage and side effects from radiation [20].
After diagnosis of an intracranial aneurysm, it is necessary to ensure the correct management and treatment of the patient. In the past, noninvasive endovascular treatment of giant aneurysms with a wide neck or fusiform aneurysms was a demanding process. Stent-assisted coiling and balloon-assisted coiling represented alternative methods of treatment for these types of aneurysms. However, studies demonstrated less expected effectiveness due to the high degree of rechanneling [25]. In recent years, flow diverters have brought about a revolution in the treatment of complex aneurysms. Their mechanism of effect is based on disrupting the blood flow from the mother artery into the aneurysm and the creation of a structure on which endothelial cells can grow, thereby isolating the aneurysm from the mother artery [26]. After implantation of an FDD the aneurysm begins to thrombolyze, shrink and collapse. Over the course of the subsequent 6–12 months following the procedure, a reconstruction of the artery and occlusion of the aneurysm takes place [25]. This therapeutic modality was used in different variants on both of our patients.
No less important is timely management and treatment of the aneurysm, from the moment of recording of symptoms of impaired vision [5,7]. We hospitalized our patients within three days of discovering their symptoms, intracranial aneurysms were identified within one week of the symptoms and treated within three months. Endovascular methods of treatment of intracranial aneurysms were used, by sequential neuroembolization treatment with implantation of a flow diverter and implantation of detachable microspirals. Thanks to the successful treatment of the aneurysms we averted the occurrence of rupture, which could have had fatal consequences for both patients. A progressive marked improvement of the finding on perimetry of the right eye was achieved in the patient from the first case report during the course of one year following treatment of the aneurysm, while in the second case report we recorded a virtually complete disappearance of the pathological finding on perimetry in both eyes after six months.
CONCLUSION
The timely identification, diagnosis and treatment of intracranial aneurysms is a serious, life-saving challenge. Thanks to the diagnostic procedure of the ophthalmologists, intracranial aneurysms were diagnosed in our patients prior to rupturing. Imaging modalities such as MRA, CTA and digital subtraction angiography fulfill an irreplaceable role in diagnosis. Endovascular methods of treatment of aneurysms with the implantation of a flow diverter appear to be a revolutionary method, with excellent postoperative results and a low perioperative risk. Upon identification of intracranial aneurysms within one week of the onset of ocular symptoms and their treatment within three months, in both our patients we achieved an improvement of the defect in the visual field over the course of 6–12 months, and in one case virtually complete disappearance.
The authors of the study declare that no conflict of interests exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company. The study has not been submitted to any other journal or printed elsewhere, with the exception of congress abstracts and recommended procedures.
Submitted to the editorial board: July 7, 2023
Accepted for publication: October 28, 2023
Available on-line: January 30, 2024
MUDr. Nora Majtánová, Ph.D.
Očná klinika SZU a UNB
Antolská 11
851 07 Bratislava
E-mail: nora.majtanova@gmail.com
Zdroje
1. Becker KJ. Epidemiology and clinical presentation of aneurysmal subarachnoid hemorrhage. Neurosurg Clin N Am. 1998;9 : 435-444.
2. Biousse V, Newman NJ. Aneurysms and subarachnoid hemorrhage. Neurosurg Clin N Am. 1999; 10 : 631-651.
3. Park JH, Park SK, Kim TH, et al. Anterior communicating artery aneurysm related to visual symptoms. J Korean Neurosurg Soc. 2009;46 : 232-238.
4. Wermer MJH, van der Schaaf IC, Algra A, Rinkel GJE. Risk of Rupture of Unruptured Intracranial Aneurysms in Relation to Patient and Aneurysm Characteristics. Stroke. 2007;38 : 1404-1410.
5. Date I, Asari S, Ohmoto T. Cerebral aneurysms causing visual symptoms: their features and surgical outcome. Clin Neurol Neurosurg. 1998;100 : 259-267.
6. Nonaka T, Haraguchi K, Baba T, Koyanagi I, Houkin K. Clinical manifestations and surgical results for paraclinoid cerebral aneurysms presenting with visual symptoms. Surg Neurol. 2007;67 : 612-619.
7. Drazin D, Choulakian A, Nuño M, et al. Improvement in Visual Symptomatology after Endovascular Treatment of Cavernous Carotid Aneurysms. J Vasc Interv Neurol. 2013;6 : 15-21.
8. McCarron M, Alberts M, McCarron P. A systematic review of Terson’s syndrome: frequency and prognosis after subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2004;75 : 491-493.
9. Kuchynka P, et al. Oční lékařství. 2nd ed. Praha: Grada; 2016. p. 936.
10. Schwedt TJ, Gereau RW, Frey K, Kharasch ED. Headache outcomes following treatment of unruptured intracranial aneurysms: a prospective analysis. Cephalalgia. 2011;31 : 1082-1089.
11. Horiuchi T, Uchiyama T, Kusano Y, et al. Penetration of the Optic Nerve or Chiasm by Anterior Communicating Artery Aneurysms: Three Case Reports, Neuro-Ophthalmology. 2011;35 : 3, 128-132.
12. Bhatti MT, Biousse V, Bose S, et al. BCSC basic and clinical science course. San Francisco: American Academy of Ophthalmology; 2020. Section 5, Neuro-ophthalmology; p. 335-347.
13. De Oliveira JG, Borba LAB, Rassi-Neto A, et al. Intracranial aneurysms presenting with mass effect over the anterior optic pathways: neurosurgical management and outcomes. FOC 2009;26:E3.
14. Vargas ME, Kupersmith MJ, Setton A, Nelson K, Berenstein A. Endovascular Treatment of Giant Aneurysms which Cause Visual Loss. Ophthalmology. 1994;101 : 1091-1098.
15. Schuss P, Güresir E, Berkefeld J, Seifert V, Vatter H. Influence of surgical or endovascular treatment on visual symptoms caused by intracranial aneurysms: single-center series and systematic review: Clinical article. J. Neurosurg. 2011;115 : 694-699.
16. Lu G, Chung J, Park JC, et al. Comparison of Visual Outcomes of Ophthalmic Artery Aneurysms Treated with Microsurgical Clipping and Endovascular Coiling. Neurointervention. 2022;17 : 18-27.
17. Ferrell AS, Lessne ML, Alexander MJ, et al. Visual Complications After Stent-Assisted Endovascular Embolization of Paraophthalmic and Suprasellar Variant Superior Hypophyseal Aneurysms: The Duke Cerebrovascular Center Experience in 57 Patients. World Neurosurg. 2012;78 : 289-294.
Štítky
OftalmológiaČlánok vyšiel v časopise
Česká a slovenská oftalmologie

2024 Číslo 1
- Pomocné látky v roztoku latanoprostu bez konzervačních látek vyvolávají zánětlivou odpověď a cytotoxicitu u imortalizovaných lidských HCE-2 epitelových buněk rohovky
- Konzervační látka polyquaternium-1 zvyšuje cytotoxicitu a zánět spojený s NF-kappaB u epitelových buněk lidské rohovky
- Dlouhodobé výsledky lokální léčby cyklosporinem A u těžkého syndromu suchého oka s 10letou dobou sledování
- Syndrom suchého oka
- Cyklosporin A v léčbě suchého oka − systematický přehled a metaanalýza
Najčítanejšie v tomto čísle
- Pars Plana Vitrectomy in the Treatment of Rhegmatogenous Retinal Detachment
- Refractive Errors Among Members of the Armed Forces of the Czech Republic
- Improvement of Visual Field Defects after Neuroembolization Treatment of Intracranial Aneurysms. Case Reports
- The Effect of Heterophoria on the Size of Distance and Near Fusion Vergence