
Free advancement ipsilateral medial plantar artery flap to encompass the entire plantar aspect of the foot – a case report and comprehensive review
Authors:
Z. Q. Lin Wu 1; B. López-Masramón 1; V. Andreu-Solà 1; J. P. Barret 1,2
Authors place of work:
Departament of Plastic and Reconstructive Surgery, Vall d’Hebrón University Hospital, Barcelona, Spain
1; Department of Surgery, School of Medicine, Universitat Autónoma de Barcelona, Barcelona, Spain
2
Published in the journal:
ACTA CHIRURGIAE PLASTICAE, 67, 2, 2025, pp. 132-136
doi:
https://doi.org/10.48095/ccachp2025132
Introduction
Skin defects in weight-bearing areas of the sole of the foot represent a surgical challenge to reconstructive surgeons. This anatomical area has unique intrinsic properties that support the full weight of the human body during standing and ambulation, such as a thicker dermis and larger and compacted subcutaneous tissue [1]. Following the reconstructive ladder, direct closure is difficult due to the poor laxity of the area, skin grafting does not provide a good reconstruction as it does not meet the previously mentioned characteristics, therefore, the use of local or free flaps, is advised [1–3]. On the other hand, most of the free flaps from other parts of the body are not able to provide quality coverage that meets the strength requirements of the sole of the foot and most local sole flaps only provide coverage for small defects.
The medial plantar artery (MPA) flap, first introduced in 1954 by Mir y Mir [4] and popularized in 1982 by Harrison and Morgan [5], is an ideal choice for reconstruction of defects in the sole, because it provides a “like with like” coverage and it is potentially sensitive [6]. Typically, it has been employed as a pedicled flap in an anterograde fashion [1,3,7] for heel reconstruction. Alternatively, it can also be used in a retrograde fashion for midfoot or forefoot defects [6,8], although this retrograde fashion entails some risks regarding the vascularization of the flap [8,9] or as a free flap for contralateral plantar reconstruction [9,10].
Traditionally, the contralateral foot is used as a donor site for free MPA flap for plantar reconstruction, but this leads to morbidity in a previously healthy foot and causes bilateral foot impairment during the postoperative state, hindering rehabilitation process [9,11]. In recent years, the use of vein grafts or distant arteriovenous pedicles to lengthen the vascular flap pedicles has become popular [12,13].
We present the case of a patient with left anterior plantar defect at the level of the head of first metatarsus after sarcoma excision. Reconstruction was performed by advancing the ipsilateral MPA flap with a greater saphenous vein pedicle extension graft.

Case report
A 30-year-old male patient with a sarcoma on the sole of the foot was referred to our hospital. In the first stage, the oncologic surgeons performed the resection, and the patient was referred to our department with a cutaneous defect of 5.5 × 3.5 cm at the level of the head of the first left metatarsus. The histopathological analysis revealed French Federation of Cancer Centers Sarcoma Group grade 1 myofibroblastic sarcoma with free margins of malignancy. The sole defect size did not allow direct closure. Since this was a young and active patient, strong, durable and sensitive coverage was needed. So, we decided to reconstruct the defect with the medial plantar artery (MPA) flap because it is the flap that provides the skin most similar to that of the defect area.
The distal part of the medial plantar pedicle was severed distally during the oncologic resection; hence retrograde flow MPA flap with distal pedicle was not an option. To avoid morbidity in the other foot, we proposed an ipsilateral sensitive MPA flap with a pedicle extension graft to reach the defect. A great saphenous vein loop obtained from the contralateral leg was used to lengthen the vascular pedicle.

Surgical technique
The patient is placed in a supine position with left hip and knee extended and externally rotated. First, we identified the posterior tibial pedicle by Doppler ultrasound (Fujifilm SonoSinte, linear probe 15 MHz) at the level of the medial malleolus and followed its course distally identifying the division in the lateral plantar artery and the medial plantar artery. We designed our 7 × 5 cm skin flap paddle centered on the course of the MPA.
We used a two-team approach. One team harvested 15 cm of the great saphenous vein in the right leg using several longitudinal incisions.
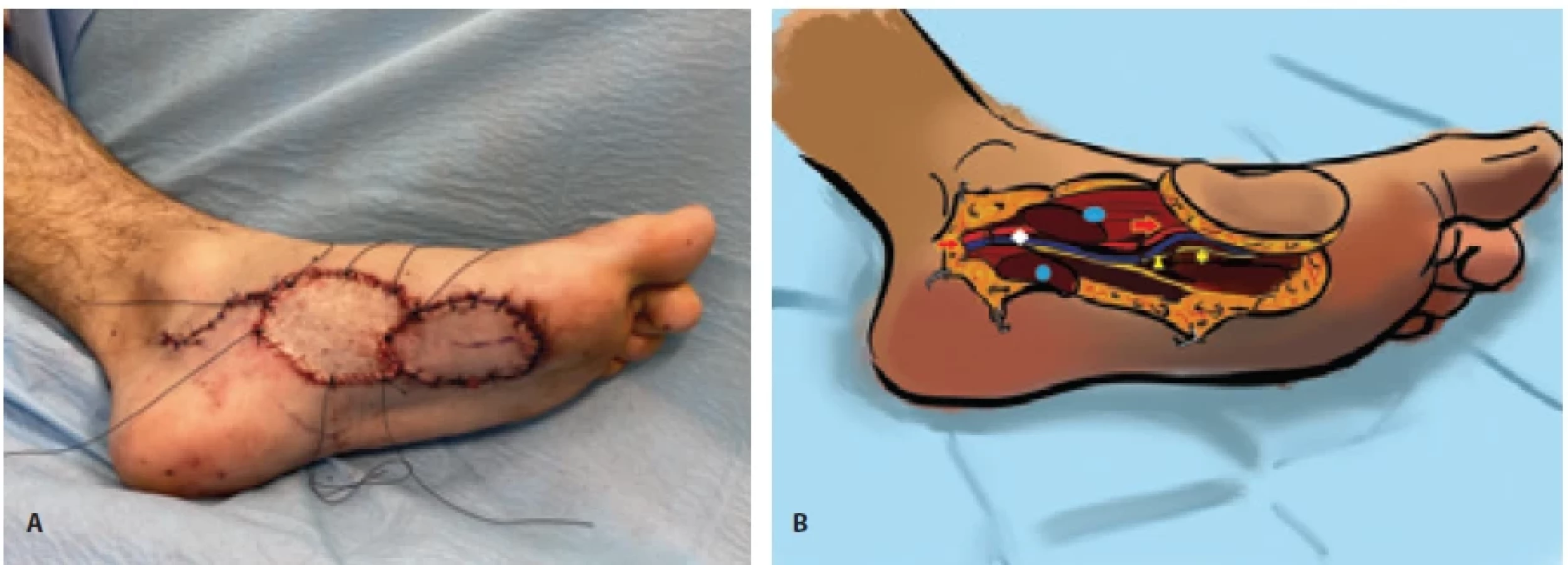
The second team elevated the left MPA flap as follows: lateral incision was made up to the muscular plane, dissection continued until the septum between the abductor hallucis and flexor digitorum brevis was reached, exposing the MPA. Once the pedicle was identified, the medial incision was performed. A subcutaneous vein was preserved in this location in case it was needed to relieve venous congestion of the flap. Next, the pedicle was dissected from distal to proximal, making a transverse section of the abductor hallucis muscle to continue the dissection up to the medial malleolus to obtain adequate vessel caliber and length. The branch of the superficial medial plantar nerve that innervates the flap was preserved, and interfascicular dissection was performed proximally. At the level of the defect, a nerve stump (corresponding to a sensory branch to the medial side of great toe of the medial plantar nerve sectioned in the primary oncologic surgery) was visualized and isolated to provide sensation to the flap (Fig. 1).
Next, the flap pedicle was detached, and anastomosis was performed. First, the proximal stump of medial plantar vessels was connected to the saphenous graft to create a venous loop (medial plantar vein (MPV) – proximal venous graft anastomosis with 2.5 mm coupler and MPA – distal venous graft anastomosis with simple 9/0 nylon stitches). Care must be taken to match the distal end of the saphenous graft with the artery and the proximal end with the vein. Correct arterial flow was verified through the vein loop. Then, the loop was severed and the anastomosis of the vein graft with the flap pedicle were performed. Positive patency test as well as optimal perfusion by indocyanine green (ICG) angiography was asseverated.
The flap was advanced to cover the defect at the level of the head of the first metatarsus and nerve coaptation was performed between the superficial branch of the medial plantar nerve of the flap and the stump that was found in the area of the defect. The flap was sutured in place with simple 4/0 nylon stitches. The donor site was closed with a full-thickness skin graft obtained from the right groin (Fig. 2). The vascular pedicle of the flap was protected by covering the proximal part with the abductor hallucis muscle (previously sectioned and now reconstructed) and the distal part was placed between the lateral head of flexor hallucis brevis and the oblique head of adductor hallucis.
The postoperative period was uneventful for the flap and dangling was performed 10 days after surgery without perfusion problems. The patient was able to fully weight-bear after 7 weeks from the tumor excision surgery. At the 9th postoperative month (Fig. 3), the patient is ambulating without difficulty and has no local complications (Suppl. material – video 1). Static two-point discrimination test was 10 mm.
Discussion
There are two pivotal milestones for the reconstruction of weight-bearing areas: first, a sufficient amount of resistant tissue is necessary to support the stress of body weight during the standing and movement. Second, the reconstruction should provide a protective sensitivity to avoid ulceration and wounds due to the pressure that the soles are subjected to [14].
The medial plantar artery flap, popularized after the description by Harrison and Morgan [5] has been postulated as one of the best options for reconstruction of the sole of the foot, since it provides “like with like” reconstruction, with sufficient amount of subcutaneous tissue to resist weight-bearing, and it can be raised as a sensate flap if the superficial branch of medial plantar nerve is preserved [13,15,16].
Typically, it has been used as an anterograde flow pedicled flap for heel reconstruction [3,15] but also as a pedicled retrograde flow flap for midfoot and forefoot coverage [6,8], as a free flap [9,10], as a pedicled MPA perforator flap [17] and even as an arterialized venous flap [18]. A systematic review performed by Opoku-Agyeman et al. [1] showed a high survival rate of pedicled flaps (98.2%), with a minor flap complication rate of 9.4% and low morbidity (5.2%).
In certain cases, such as traumatic or oncologic patients where the distal portion of the MPA has been damaged due to trauma or resection, it is not possible to perform a retrograde flow pedicled MPA flap for coverage of midfoot or forefoot area. In these patients, reconstructive surgeons could perform a “like with like” coverage with a free contralateral MPA flap, however, this implies morbidity in a healthy foot and hinders postoperative rehabilitation due to bilateral foot involvement.
Paget et al. [11] suggest that patients have a weaker push-off from the great toe of the donor site after an MPA transfer. Besides this, Karagawa et al. [9] performed a gait analysis in a patient with a free MPA flap for the coverage of the contralateral sole defect, where a balanced gait was evidenced in both the reconstructed and donor foot.
Methods to elongate the pedicles of the flaps have been used for years to reach adequate recipient vessels, since the defect area may have history of radiation, trauma or malignancy that cause a poor condition of nearby recipient vessels or an absence of them [12,13]. The most common method to elongate pedicles is using vein grafts such as the great saphenous vein, although interposition arteriovenous (AV) grafts such as the descending branch of the lateral circumflex femoral or deep inferior epigastric vessels were also described [19,20]. The main problem associated with AV grafts is the sacrifice of a potential flap that may be needed in the future, therefore, it is recommended to use vein grafts in anticipation of needing any of the vascularized flaps supplied by the vascular pedicle intended to elongate our flap pedicle [21].
Classically, it has been considered that the use of venous grafts increases the risk of flap failure due to thrombosis, although several studies show controversial results [22–26], having to consider other factors related to the patient, such as arteriosclerosis or radiation [27,28]. We maintain that, if a proper microsurgical technique is used, extension vein grafts do not entail a significantly higher complication rate.
In our case, the distal vascular axis of the MPA was affected by the oncologic surgery, therefore we ruled out a retrograde flow MPA flap in first instance. We also discarded the use of the contralateral MPA flap to avoid morbidity in the healthy foot of a young and active patient. Therefore, we used a great saphenous vein loop to “advance” the MPA flap in the same foot. We consider that this is a simple and reproducible method that allow reconstructive surgeons to provide optimal coverage of defects in any location of the entire sole of the foot with an antegrade flow MPA flap, without the mobility and range limitations of a pedicled MPA flap and without the involvement of the contralateral foot.
Conclusion
The utilization of the extended pedicle MPA flap with anterograde flow provides a sensitive “like with like” coverage, that has potential to encompass defects in the entire sole of the foot, without compromising the contralateral foot as a donor site and without the risk of vascular impairment of retrograde flow MPA flaps. Although further clinical investigations will be required to make robust conclusions, this method would be a suitable solution to cover defects in weight-bearing areas in the plantar aspect of the foot.
Disclosures: The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.Data availability statement: The data that support the findings of this study are available from the corresponding author, ZQLW, upon reasonable request.
Roles of authors: Zhan Q. Lin Wu – conceptualization, writing (original draft), review and editing, visualization; Bernat López-Masramón – conceptualization, visualization, supervision; Víctor Andreu-Solà – conceptualization, visualization, supervision; Juan P Barret – conceptualization, visualization, supervision.
| For supplementary material (video 1), see the online version of the article at www.achp.cz. |
Zdroje
Štítky
Chirurgia plastická Ortopédia Popáleninová medicína TraumatológiaČlánok vyšiel v časopise
Acta chirurgiae plasticae
2025 Číslo 2
- Liečba bolesti po jednodňovej chirurgii
- Fixní kombinace tramadol/paracetamol je doporučenou volbou v léčbě chronické bolesti v ordinaci praktického lékaře
- Kombinace kodein/paracetamol prokázala stejný analgetický účinek jako hydrokodon/paracetamol
- Nová metoda kombinované analgetické léčby vychází z multimechanistické povahy bolesti
- Léčba chronické bolesti u starších pacientů vychází z farmakologických i nefarmakologických přístupů
Najčítanejšie v tomto čísle
- Mini-invasive temporalis muscle tendon transfer and lengthening temporalis myoplasty for facial reanimation – a retrospective outcome analysis
- Limb saving with regenerative medicine tactics – a case report
- Risk factors for cleft lip and palate in the Czech population – a double center study
- Surgical management of accessory breast tissue: liposuction and mastectomy in axillary localization – a case series