
Maternal and fetal outcomes in subsequent pregnancies of patients who underwent Acar-style conservative surgery for placenta accreata spectrum
Mateřské a fetální výsledky u následujících těhotenstvích pacientek, které podstoupily konzervativní operaci typu Acar pro spektrum placenty accreta
Cíl: Tato studie si klade za cíl porovnat mateřské a fetální výsledky u následujících těhotenství pacientek, které podstoupily konzervativní (fertilitu šetřící) operaci placenta accreta spektra (PAS) a současných těhotenství pacientek po předchozím císařském řezu. Jeho cílem je zhodnotit proveditelnost konzervativní operace. Metody: Studie byla provedena v období od ledna 2011 do září 2021 na Porodnicko-gynekologické klinice Necmettin Erbakan University Meram Medical University Hospital. Soubory pacientek, které podstoupily segmentální resekci dělohy s diagnózou PAS a poté znovu otěhotněly a které podstoupily císařský řez, byly retrospektivně naskenovány z nemocničního systému elektronických záznamů pacientek bez diagnózy PAS, ale s alespoň jednou předchozí anamnézou. Císařský řez. Výsledky: Gestační týden, porodní hmotnost, intrauterinní růstová retardace a hodnoty APGAR byly porovnány s ohledem na výsledky plodu a mezi těmito dvěma skupinami nebyl nalezen žádný statisticky významný rozdíl. Sedm pacientek ve studijní skupině a jedna pacientka v kontrolní skupině vyžadovalo poporodní transfuzi (p = 0,026), infekce močových cest byly častější u pacientek s PAS v anamnéze (p = 0,038). Závěr: I když je císařský řez standardní léčebnou metodou v případech anomálie placentární invaze, konzervativní (uterus šetřící) operace se zdá být použitelná u pacientek s fertilitou i přes chirurgické komplikace. Konzervativní operace typu acar je důležitá jak z hlediska zachování fertility u PAS.
Klíčová slova:
spektrum placenta accreta – konzervativní operace – perinatální výsledek
Authors:
N. Şengül 1
![]() ; F. Yağbasan 2
; F. Yağbasan 2
![]() ; A. Acar 3
; A. Acar 3
![]()
Authors place of work:
Dr. Ali Kemal Belviranlı Maternity and Children‘s Hospital, Konya, Turkey
1; Private Konya Farabi Hospital, Konya, Turkey
2; Department of Obstetrics and Gynecology, Necmettin Erbakan University Medical School of Meram, Konya, Turkey
3
Published in the journal:
Ceska Gynekol 2023; 88(5): 328-333
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg2023328
Summary
Objective: This study aims to compare the maternal and fetal outcomes in subsequent pregnancies of patients who underwent conservative surgery (fertility-sparing) for placenta accreta spectrum (PAS) and the current pregnancies of patients who had a previous cesarean section. It aims to evaluate the feasibility of conservative surgery. Methods: The study was carried out between January 2011 and September 2021 at the Gynecology and Obstetrics Clinic of Necmettin Erbakan University Meram Medical Faculty Hospital. The files of patients who underwent uterine segmental resection surgery with the diagnosis of PAS and then became pregnant again and who underwent cesarean section were retrospectively scanned from the hospital electronic registry system of patients without a PAS diagnosis but with a history of at least one previous cesarean section. Results: Gestational week, birth weight, intrauterine growth retardation, and APGAR values were compared regarding the fetal outcomes and no statistically significant difference was found between the two groups. Seven patients in the study group and one patient in the control group required postpartum transfusions (P = 0.026), and urinary system infections were more frequent in patients with a history of PAS (P = 0.038). Conclusion: Although cesarean hysterectomy is the standard treatment method in cases of placental invasion anomaly, conservative (uterus-sparing) surgery seems to be applicable in fertile patients despite surgical difficulties. Acar-style conservative surgery is important in terms of both fertility preservation in PAS cases.
Keywords:
placenta accreta spectrum – conservative surgery – perinatal outcome
Introduction
Placenta accreata spectrum (PAS) describes abnormal decidualization and invasion associated with damage to the previously formed endometrium--myometrium interface [1]. PAS defines placental adhesion anomalies, including placenta accreata, increta, and percreta [2]. Placenta accreata includes superficial myometrial invasion, while placenta increta includes deep myometrial invasion, and placenta percreta includes full-thickness myometrial invasion and sometimes involvement of the uterine serosa and adjacent organs [3]. The incidence of the placenta accreta spectrum increases in proportion to the number of previous cesarean deliveries in placenta previa patients. In the presence of placenta previa, the probability of PAS presence in patients with a previous cesarean (C/S) is 3%, while the ratio is 11% in those with two previous C/S, 40% in those with three previous C/S, 61% in patients with four previous C/S, and 67% in patients with a previous history of 5 or more C/S [4]. Other risk factors that increase the risk of PAS are increased number of births, maternal age, previous uterine surgeries, and endometrial damage.
The primary treatment modalities for PAS are cesarean hysterectomy, manual removal of the attached placenta, or a conservative approach. Of these approaches, manual removal of the placenta is associated with increased postpartum bleeding, while the conservative approach is associated with intra-abdominal sepsis, the need for hysterectomy, and postpartum hemorrhage [5]. Severe hemorrhages can be seen at birth in patients with severe invasion anomalies, which carries a high risk of mortality and morbidity. If the diagnosis is clarified intraoperatively in patients with a pre-diagnosis of PAS, the recommended treatment is peripartum hysterectomy. However, in the literature, there are many published case reports in which fertility-preserving methods without hysterectomy are applied [6,7]. The American College of Obstetricians and Gynecologists (ACOG) recommends planned C/S hysterectomy starting from the 35th week in the presence of PAS [8]. However, due to our country‘s sociodemographic characteristics, families with a low number of live children, despite repeated cesarean section operations or who do not want to lose their fertile characteristics, demand fertility-preserving treatment. In this context, a fertility-preserving approach was applied to the selected patients in our clinic.
Our study aims to evaluate the feasibility of conservative (fertility-preserving) surgery by comparing the maternal and fetal outcomes in subsequent pregnancies of patients who underwent conservative (fertility-preserving) surgery due to PAS in our clinic with the results of the patients who only had a previous cesarean section and then became pregnant again.
Materials and methods
The files of patients with a history of uterine segmental resection surgery due to PAS diagnosis, who subsequently became pregnant again and underwent C/S, and patients without PAS diagnosis but with a history of at least one previous C/S and repeated C/S between January 01, 2011 and September 01, 2021 at the Gynecology and Obstetrics Clinic of Necmettin Erbakan University Meram Medical Faculty Hospital, were retrospectively scanned from the hospital‘s electronic registry system. Approval for this study was obtained from the Ethics Committee of Necmettin Erbakan University Meram Faculty of Medicine, Non-Pharmaceutical and Medical Device Research (Ethics committee decree dated 13. 5. 2022 – numbered 2022/3790). The patients included in the control group consisted of subsequent cesarean sections of patients who were not diagnosed with any placental invasion anomaly preoperatively or intraoperatively. Pregnant women under 18 years of age, grand multiparous with myoma uteri, severe anemia (Hg < 10 gr/dL), multiple pregnancies, macrosomic babies (EFW ≥ 4,500 gr) and using anticoagulant (LMWH – low molecular weight heparin) were excluded from the study. The diagnosis of placental invasion was made in our clinic using abdominal, vaginal, and Doppler ultrasonography. Invasion anomaly was diag - nosed by the presence of one or more of the findings, such as the presence of large lacunae in the placental area, the disappearance of the retroplacental hypoechogenic region, thinning of the retroplacental myometrial distance, hypervascularization between the lower uterine segment and the bladder and turbulent flow in the lacuna during the Doppler evaluation. Postoperatively, all placentas were sent to pathology, and the diagnosis of invasion anomaly was confirmed histologically. The surgery preferred by our clinic in PAS cases is the uterus-preserving approach. After spinal anesthesia, patients are placed in the lithotomy position by the urology team, and bilateral ureteral catheters are placed under the guidance of a cystoscope, followed by a midline incision below and above the umbilicus. The uterine cavity is entered through a vertical fundus incision. The bladder flap is dissected from the uterus‘s anterior surface by ligature starting from the paracervical area. Until the ureteral catheter is felt in both broad ligaments, a window is opened via ligature, and the uterus is devascularized with a clamp placed on the cervicoisthmic region of the uterus. After the uterine segment with the placental bed is resected, placental bed sutures are placed, the uterus is closed, and the procedure is terminated. In cases with bladder invasion, the bladder is opened in a controlled manner, the placental tissue is cleaned, and the bladder is repaired after the necessary bleeding control is performed. Leakage from the bladder is checked with methylene blue. Age, gestational week, gravida, parity, number of abortions, number of curettages, number of cesarean sections, and time passed until the next pregnancy were recorded from the demographic characteristics of the patients. Admission to the hospital due to abortion imminence, oligohydramnios, polyhydramnios, preeclampsia, urinary tract infection, and intrauterine growth retardation were evaluated as obstetric outcomes. Postpartum hemorrhage, preoperative hemoglobin, postoperative hemoglobin, postoperative hospital stay duration, transfusion need, fetal APGAR score, and birth weights were recorded and analyzed statistically.
Statistical analysis
All data collected for statistical analysis were transferred to the computer environment and analyzed with the SPSS (Statistical Package for Social Sciences) v.18.0 package program. In descriptive analyses, frequency data were presented as numbers (N) and percentages (%), while numerical data were given using the arithmetic mean ± standard deviation (sd), median (1st quartile–3rd quarter), and minimum-maximum. Chi-square (C2) test and Fisher‘s exact Chi-square test were used to compare categorical data. Compliance of numerical data with a normal distribution was examined with the Shapiro-Wilk test. Mann-Whitney U-test was used to compare the two groups for numerical variables that do not comply with the normal distribution. The statistical significance level was considered as P < 0.05 in all tests.
Results
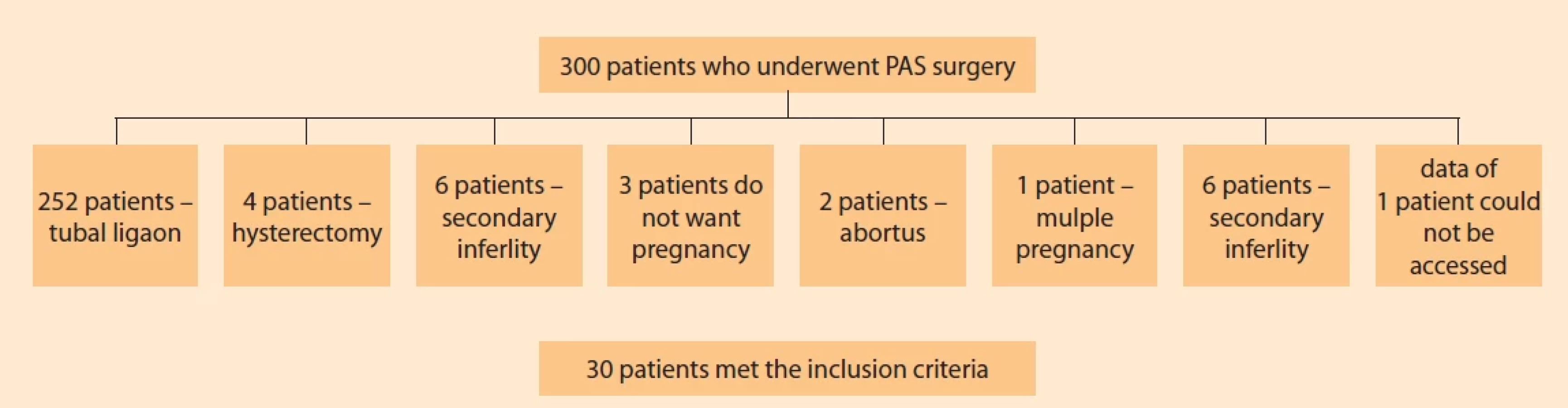
PAS surgery was applied to a total of 300 patients in our clinic, and tubal ligation was applied to 252 (84%) patients during cesarean section. Four patients (1.33%) underwent a hysterectomy in the same session due to hemorrhage. Of the remaining 44 patients (14.66%), three cases (6.81%) were patients with no pregnancy will. Of the remaining 41 patients, six (14.63%) patients were excluded due to secondary infertility, two patients (4.87%) had an abortion, one patient (2.43%) had an ectopic pregnancy, one patient (2.43%) had multiple pregnancies, and the data could not be obtained for one patient (2.43%) (Fig. 1). The remaining 30 patients with a history of PAS surgery became pregnant and had a cesarean section, and 30 control patients with a history of PAS who had a history of cesarean section and who underwent elective cesarean section were included in the study by matching one-on-one. Age, number of pregnancies, number of parity, number of abortions, number of C/S, and the number of revision curettage (R/C) of the patients in the group with a history of PAS were significantly higher than those in the group without the mean (P = 0.005; P = 0.001; P = 0.001; P = 0.001; P = 0.001; P = 0.001; respectively). Demographic data of all patients are given in Tab. 1. When the invasion anomaly was diagnosed during pregnancy, abortion imminence history, amniotic fluid index abnormality, preeclampsia diagnosis, and hospital stay periods were evaluated in the groups with and without PAS history, and no statistical difference was observed between the two groups (P > 0.05). Considering the postpartum transfusion needs, seven (23.3%) patients in the study group and one (3.3%) patient in the control group had transfusion needs (P = 0.026) (Tab. 2). Gestational week, birth weight, intrauterine growth retardation, and APGAR values were compared regarding the fetal outcomes and no statistically significant difference was found between the two groups (Tab. 3). After comparing the development of urinary tract infection in pregnancies with a PAS history with that of pregnant women without a PAS history, urinary tract infection was observed more frequently in patients in the PAS group (P = 0.038). The need for blood transfusion during surgery was significantly higher in the group with a PAS history than in the group without PAS (P = 0.026). Postoperative hemoglobin values were significantly lower in the study group (9.9 gr/dl ± 2.03 vs. 10.88 ± 1.18; P = 0.025).

Discussion
Increased cesarean section rates and curettage rates due to recurrent pregnancy losses cause an increase in patient groups diagnosed with placental invasion anomaly worldwide. Even if the patients have a previous cesarean section, the possibility of placenta invasion anomaly increases in the presence of placenta previa. In addition, severe forms of placental invasion anomaly seem to appear in younger patients and cause them to have fewer children in the future. In our clinic, Ali Acar et al performed Acar-style conservative surgery in which the uterus was preserved with a modified Acar-suture technique by removing the placenta and invading myometrium tissue as a fertility-sparing surgery, which was published previously [9]. Our surgical success rate was 94%. The rate of babies taken home after PAS surgery was 73.1%.
The current cesarean rate in Turkey is approximately 53% [10]. Physicians should expect to encounter an increasing rate of placental invasion anomalies in the coming years. Finding an applicable and reliable method to manage such anomalies will be important, considering the importance of fertility in our country and the world. Various conservative approaches have been described for the treatment of placental invasion anomaly. Palacios-Jaraquemada et al reported that they performed uterine repair in patients with anterior placenta percreta by providing hemostasis with selective vascular ligation or surgical myometrial compression methods. The anterior wall defect was repaired using myometrial cross-sutures as the primary suture, and in their case series, they reported that they applied a fibrin adhesive and polyglycolic mesh, and a non-adherent cellulose layer over this reconstruction. The rate of uterus preservation was 73.5% [11]. In the retrospective study of Karaman et al, it was stated that local resection could be an effective and safe alternative to cesarean hysterectomy in cases of placenta percreta [12]. Kılıçcı et al successfully treated cases with placenta percreta with partial resection in selected cases. In their study, in which they examined segmental resection of the anterior wall of the uterus and the modified minimally invasive uterus-preserving surgery technique to preserve fertility in cases with placenta percreta, they successfully applied the modified segmental resection technique to 11 pregnant women who were confirmed to have placenta previa and placenta percreta [13].


The long-term fertility prognosis of women treated with conservative treatment for placenta accreta has been a matter of concern for patients wishing to preserve their fertility. In the 2010 study of Provansal et al, despite the preservation of the uterus, most women did not express a desire for another pregnancy, possibly due to the psychological trauma related to childbirth. Recurrence of placenta accreta was observed in 2 out of 15 pregnancies after conservative treatment for placenta accreta [14]). In our case series, the number of cases who did not have a tubal ligation and did not want pregnancy was 6–8%. The study by Sentilhess et al suggests that successful conservative treatment for placenta accreta does not compromise patients‘ subsequent fertility or obstetric outcomes, but there is a high risk of placenta accreta recurrence during future deliveries. However, out of 96 women under follow-up after successful conservative treatment, severe intrauterine synechia, known to affect fertility adversely, was found in eight women who did not continue to menstruate. This relatively high rate of synechiae following placenta accreta is consistent with a previous smaller and more limited study suggesting that placenta accreta may be a risk factor for synechia [15]. Pineless et al obtained successful results in six (55%) cases out of 11 cases with placenta accreta spectrum that they followed by leaving the placenta in place, and they performed minimally invasive hysterectomy in four cases and abdominal hysterectomy in one case. Of the six patients whose uterus was preserved, four became pregnant, three of them had a healthy term pregnancy, and one had a 19-week abortion [16]. In the study of Huang et al, the placenta was left in place for 21 patients after transcatheter artery embolization, and conservative treatment was applied; four patients underwent a hysterectomy, 16 patients returned to their normal menstrual cycle, and one patient had a healthy term pregnancy [17]. There are studies related to the decrease in ovarian reserve, and thus, fertility when compared with the same age group after conservative PAS surgery performed by applying uterine artery embolization [18].
Our study has some limitations. First of all, the study was designed as a retrospective study. The number of patients in the study group was low, and most cases with PAS request tubal ligation; therefore, the study group does not reflect the general population PAS cases, and there is no comparison of long-term reproductive results with other conservative methods.
Techniques applied in conservative surgery vary depending on the surgeon‘s experience and the patient‘s intraoperative clinical outcome. Although cesarean hysterectomy is the standard treatment method for placental invasion anomaly cases, conservative (uterus-preserving) surgery seems to be applicable for patients who want to become pregnant despite surgical difficulties. Acar-style conservative surgery is both effective in terms of fertility preservation and helpful in preventing hysterectomy in PAS cases.
Authorship
NŞ: study design, patient management, and manuscript writing/editing, data collection
FY: data analysis, patient management
AA: data analysis, patient management, contributed to and approved of the final version of the manuscript
Submitted/Doručeno: 11. 5. 2023
Accepted/Přijato: 18. 5. 2023
Nurullah Şengül, MD
Dr. Ali Kemal Belviranlı Maternity
and Children‘s Hospital
Yunus Emre, Akyokuş Street
42080 Meram/Konya
Turkey
akkus1987@gmail.com
Zdroje
1. Dogru S, Akkus F, Atci AA et al. The fetal and maternal outcomes related to previous number of cesarean sections and uterus sparing surgery in women with abnormal placentation. J Clin Invest Surg 2022; 7 (1): 25–30.
2. Dogru S, Atci AA, Akkus F et al. Use of ureteral catheter in uterine-sparing surgery for placenta accreta. Perinat J 2022; 30 (2): 158–164. doi: 10.2399/prn.22.0302009.
3. Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: twenty-year analysis. Am J Obstet Gynecol 2005; 192 (5): 1458–1461. doi: 10.1016/j.ajog.2004.12.074.
4. Harris RL, Cundiff GW, Theofrastous JP et al. The value of intraoperative cystoscopy in urogynecologic and reconstructive pelvic surgery. Am J Obstet Gynecol 1997; 177 (6): 1367–1371. doi: 10.1016/s0002-9378 (97) 70077-2.
5. Eller AG, Porter TF, Soisson P et al. Optimal management strategies for placenta accreta. BJOG 2009; 116 (5): 648–654. doi: 10.1111/j.1471-05 28.2008.02037.x.
6. Spiliopoulos M, Kareti A, Jain NJ et al. Risk of peripartum hysterectomy by mode of delivery and prior obstetric history: data from a population-based study. Arch Gynecol Obstet 2011; 283 (6): 1261–1268. doi: 10.1007/s0040 4-010-1554-6.
7. Tam Tam KB, Dozier J, Martin JN Jr. Approaches to reduce urinary tract injury during management of placenta accreta, increta, and percreta: a systematic review. J Matern Fetal Neonatal Med 2012; 25 (4): 329–334. doi: 10.3109/14767058.2011.576720.
8. Jauniaux E, Kingdom JC, Silver RM. A comparison of recent guidelines in the diagnosis and management of placenta accreta spectrum disorders. Best Pract Res Clin Obstet Gynaecol 2021; 72 : 102–116. doi: 10.1016/j.bpobgyn.2020.06.007.
9. Acar A, Ercan F, Pekin A et al. Conservative management of placental invasion anomalies with an intracavitary suture technique. Int J Gynaecol Obstet 2018; 143 (2): 184–190. doi: 10.1002/ijgo.12593.
10. OECD. Caesarean sections. 2013 [online]. Available from: https: //data.oecd.org/healthcare/caesarean-sections.htm.
11. Jaraquemada JM, Pesaresi M, Nassif JC et al. Anterior placenta percreta: surgical approach, hemostasis and uterine repair. Acta Obstet Gynecol Scand 2004; 83 (8): 738–744. doi: 10.1111/j.0001-6349.2004.00517.x.
12. Karaman E, Kolusarı A, Çetin O et al. Local resection may be a strong alternative to cesarean hysterectomy in conservative surgical management of placenta percreta: experiences from a tertiary hospital. J Matern Fetal Neonatal Med 2017; 30 (8): 947–952. doi: 10.1080/14767058.2016.1192119.
13. Kilicci C, Sanverdi I, Ozkaya E et al. Segmental resection of anterior uterine wall in cases with placenta percreta: a modified technique for fertility preserving approach. J Matern Fetal Neonatal Med 2018; 31 (9): 1198–1203. doi: 10.1080/14767058.2017.1311862.
14. Provansal M, Courbiere B, Agostini A et al. Fertility and obstetric outcome after conservative management of placenta accreta. Int J Gynaecol Obstet 2010; 109 (2): 147–150. doi: 10.1016/j.ijgo.2009.12.011.
15. Sentilhes L, Kayem G, Ambroselli C et al. Fertility and pregnancy outcomes following conservative treatment for placenta accreta. Hum Reprod 2010; 25 (11): 2803–2810. doi: 10.1093/humrep/deq239.
16. Pineles BL, Coselli J, Ghorayeb T et al. Leaving the placenta in situ in placenta accreta spectrum disorders: a single center case series. Am J Perinatol 2022. doi: 10.1055/a-1885-1942. Online ahead of print.
17. Huang KL, Leung-Chit Tsang L, Cheng YF et al. Planned conservative management of placenta increta and percreta with prophylactic transcatheter arterial embolization and leaving placenta in situ for women who desire fertility preservation. Placenta 2020; 97 : 51–57. doi: 10.1016/j.placenta.2020.06.003.
18. Mohr-Sasson A, Spira M, Rahav R et al. Ovarian reserve after uterine artery embolization in women with morbidly adherent placenta: a cohort study. PloS One 2018; 13 (11): e0208139. doi: 10.1371/journal.pone.0208 139.
Štítky
Detská gynekológia Gynekológia a pôrodníctvo Reprodukčná medicínaČlánok vyšiel v časopise
Česká gynekologie
2023 Číslo 5
- I „pouhé“ doporučení znamená velkou pomoc. Nasměrujte své pacienty pod křídla Dobrých andělů
- Gynekologické potíže pomáhá účinně zvládat benzydamin
- Mýty a fakta ohledně doporučení v těhotenství
- Jak podpořit využití železa organismem bez nežádoucích účinků
- Gynekologové a odborníci na reprodukční medicínu se sejdou na prvním virtuálním summitu
Najčítanejšie v tomto čísle
- Včasná léčba synechie vulvy v dětském věku – prevence pozdních komplikací
- Relugolix kombinovaná terapie a symptomy děložní myomatózy – vybrané kazuistiky indikačního spektra a výsledků léčby
- Implementace ERAS protokolu v gynekologii a onkogynekologii – zhodnocení pilotní studie
- Rodící se myom jako příčina močové retence