
Efficacy of pectoral nerve block type II versus thoracic paravertebral block for analgesia in breast cancer surgery
Efektivita blokády pektorálneho nervu typu II oproti torakálnej paravertebrálnej blokáde v analgézii po operácii tumoru prsníka
Východiská: Ultrazvukom riadená blokáda pektorálneho nervu typu II je v súčasnosti používaná technika pooperačnej analgézie po operácii tumoru prsníka. Po desaťročia sa na tento účel využívala torakálna paravertebrálna blokáda. Táto práca ponúka porovnanie týchto dvoch spomenutých techník v manažmente pooperačnej analgézie.
Materiál a metódy: Šesťdesiat dospelých žien podstúpilo unilaterálnu radikálnu mastektómiu alebo kvadrantektómiu s axilárnou disekciou. Pacientkam (randomizované) bola vykonaná buď blokáda pektorálneho nervu s aplikáciou 30 ml ropivakaínu 0,375% (skupina Pecs) alebo torakálna paravertebrálna blokáda s aplikáciou ropivakaínu 20 ml 0,5% (skupina TPVB). Posudzované premenné boli intenzita bolesti po operácii, podľa numerickej hodnotiacej stupnice, po 0, 2, 4, 6, 12, 18 a 24 hodinách, 24-hodinová pooperačná spotreba opioidných analgetík (promedol) a neopioidov (ketoprofén) a časový interval po podaní prvého potrebného analgetika.
Výsledky: Neboli zistené žiadne štatisticky významné rozdiely v intenzite bolesti u pacientok po operácii. Desať pacientok (33%) zo skupiny Pecs a deväť pacientok (33%) zo skupiny TPVB nepožadovalo aplikáciu žiadneho analgetika počas prvých 24 hodín (p = 0,793). Priemerná spotreba ketoprofénu po operácii bola nižšia v skupine Pecs, a to 63,3 (± 66,87) mg oproti 90,0 (± 84,49) mg (p = 0,283). Počet pacientok, ktoré požadovali promedol bol 6 (20 %) v skupine Pecs a 8 (27 %) v skupine TPVB. Časový interval do podania prvého analgetika bol dlhší v skupine Pecs, tj. 550 (400,0–600,0) min, oproti skupine TPVB, tj. 510 (360,0–600,0) min (p = 0,506).
Záver: Blokáda pektorálneho nervu typu II po operácii tumoru prsníka s aplikáciou ropivakaínu 0,375% môže poskytnúť porovnateľnú pooperačnú analgéziu ako jednostupňová torakálna paravertebrálna blokáda.
Autoři deklarují, že v souvislosti s předmětem studie nemají žádné komerční zájmy.
Redakční rada potvrzuje, že rukopis práce splnil ICMJE kritéria pro publikace zasílané do biomedicínských časopisů.
Klíčová slova:
torakálna paravertebrálna blokáda – blokáda pektorálneho nervu – chirurgia prsníka
Authors:
Volodymyrovych Volodymyr Martsiniv 1,2; Anatoliiovych Oleg Loskutov 1; Mykolaiovych Andriy Strokan 1,2; Mykolaiovych Maksim Pylypenko 1; Volodymyrovych Mihailo Bondar 1
Authors place of work:
Department of Anaesthesia and Intensive Care, P. L. Shupyk National Medical Academy of Postgraduate Education, Kyiv, Ukraine
1; Department of Anaesthesia and Intensive Care, Feofaniya Clinical Hospital of State Management of Affairs, Kyiv, Ukraine
2
Published in the journal:
Klin Onkol 2020; 33(4): 296-301
Category:
Původní práce
doi:
https://doi.org/10.14735/amko2020296
Summary
Background: Ultrasound-guided pectoral nerve block type II is a recently proposed technique for postoperative analgesia after breast cancer surgery. The thoracic paravertebral block is widely used for this purpose by decades. The presented study compares the efficacy of these two techniques for postoperative analgesia.
Materials and methods: Sixty adult women were undergoing unilateral radical mastectomy or quadrantectomy with axillary dissection. The patients were randomized to receive either pectoral nerve block with 30 ml ropivacaine 0.375% (Pecs group) or thoracic paravertebral block with 20 ml ropivacaine 0.5% (TPVB group). The evaluated variables included pain intensity by the numerical rating scale at 0, 2, 4, 6, 12, 18 and the 24 hours, 24-hour postoperative opioid (promedol) and nonopioid (ketoprofen) consumption and the time to first rescue analgesia.
Results: There were no statistically significant differences between both groups in the pain intensity after surgery. Ten (33%) patients from Pecs group and nine (30%) patients from TPVB group did not require any analgesia within the first 24 hours (P = 0.793). The mean postoperative ketoprofen consumption was lower in Pecs group: 63.3 (± 66.87) mg vs. 90.0 (± 84.49) mg (Р = 0.283). The number of patients who required promedol was 6 (20%) vs. 8 (27%) in Pecs and TPVB groups, respectively (Р = 0.542). The time to first analgesic request was longer in Pecs group, 550 (400.0–600.0) min vs. 510 (360.0–600.0) min (Р = 0.506) in TPVB group.
Conclusions: In breast cancer surgery, the pectoral nerve block type II with ropivacaine 0.375% can provide postoperative analgesia that is comparable to the single-level thoracic paravertebral block.
Keywords:
thoracic paravertebral block – pectoral nerve block – breast surgery
Background
Breast cancer is the most frequently diagnosed malignancy among women in the regions with different economic development with an estimated 1.67 mil. new cancer cases diagnosed in 2012 [1]. In Ukraine, these cancers are also the first most common malignancies among women. In the last decades, its incidence has increased [2]. The main surgical method of the treatment of operable breast cancer is organ-sparing surgery with lymph node dissection. Despite the variety of the methods of analgesia, up to 40% of women suffer from acute pain after this surgery [3]. There is a high risk of chronic pain development after this surgery [4]. Therefore, the research and development of safe analgesia techniques for these interventions remain a topic of interest.
Thoracic epidural analgesia, paravertebral and intercostal nerve blocks have been effectively used during several decades for analgesia in breast surgery. The thoracic paravertebral block (TPVB) provides good perioperative analgesia [5], and it can be used even as monoanaesthesia when the block is performing at multiple vertebral levels [6]. The main disadvantage of this method is the risk of serious complications, such as pneumothorax and administration of local anaesthetic in the subarachnoid space. The widespread use of the ultrasound visualization for the peripheral nerve blockade has given an impetus to the development of new, minimally invasive myofascial blocks, such as pectoral nerve block type II (Pecs block).
Several randomized controlled trials compared postoperative analgesia after Pecs block with TPVB for breast cancer surgery. Some studies show that Pecs block reduces the need for opioid analgesics in the postoperative period compared with TPVB [7–9]. On the other hand, some studies have shown that TPVB has a more powerful analgesic effect than Pecs block [10,11]. Versyck et al performed a meta-analysis of five studies which shows that the analgesic effect of these two methods is comparable [12]. A similar conclusion was made by Tripathy et al when comparing these two techniques for opioid-free anaesthesia for breast cancer surgery [13]. Such different results were obtained because the researchers used different kinds and volumes of local anaesthetic and different block technique. In most trials, 0.25% bupivacaine [11,14,17] or 0.25% levobupivacaine [7,12] were used as local anaesthetics. Tripathy et al mixed 0.25% bupivacaine with 2% lignocaine and with adrenaline and 1 μg/kg dexmedetomidine [13]. In the study by Kulhari et al, ultrasound-guided Pecs block provided better analgesia in the postoperative period than TPVB in patients undergoing modified radical mastectomy [8]. Both blocks were performed with 25 ml ropivacaine 0.5%. There were trials and case reports where Pecs block was effective for postoperative analgesia with a lower concentration of ropivacaine [15,16]. This study aimed to compare the efficacy of pectoral nerve block type II with 30 ml ropivacaine 0.375% and thoracic one level paravertebral block with 20 ml ropivacaine 0.5% for analgesia after breast cancer
surgery.
Materials and methods
The study was conducted from January 2018 to May 2019 in the Feofaniya Clinical Hospital. The work plan was approved by the institutional ethics committee, reference No. 8, dated October 23, 2017. Female patients in the age group of 18–80 years with ASA grade I–II breast cancers, who were undergoing elective mastectomy or quadrantectomy with axillary lymph node dissection, were included in this study. Exclusion criteria: allergy to local anaesthetics, the body mass index of more than 35 kg/m2, pregnancy, chronic pain in the arm and/or chest, required use of painkillers and/or other medications to treat chronic pain, previous operations on this mammary gland and/or received radiotherapy, use of anticoagulants or bleeding disorders and skin inflammation at the local anaesthetic injection site.
The patients were randomized by sealed envelope method into two groups: pectoral nerve block (Pecs group) and paravertebral block (TPVB group). The perioperative procedures in both groups were similar and consistent with the Feofaniya Hospital’s local protocols for this type of surgery. After admission to the operating room, venous access and standard monitoring including pulse oximetry, non-invasive blood pressure measurement, ECG and capnography were established for the patient. After establishing a peripheral intravenous line, diazepam 5 mg and non-steroidal anti-inflammatory drug (ketoprofen 100 mg) were administered for premedication. Then the appropriate block was performed in aseptic settings and under ultrasound guidance.
The pectoral nerve block was performed with the technique described by Blanco et al [17]. The ultrasound machine “General electric Logiq E” (GE Healthcare, LittleChalfont, United Kingdom) with a linear probe (8–15 MHz) was used to visualize the anatomical structures. The ultrasound probe was placed in the subclavian area perpendicular to the middle of the clavicle, where we visualized the pectoral muscles (major and minor). Then we moved the probe toward the armpit and at the level of the 4th rib until achieving the optimal ultrasound image. After that, in the aseptic settings and after skin infiltration with anaesthesia with lidocaine 1%, we injected 20 ml ropivacaine 0.375% between the pectoralis minor and serratus anterior muscles, using an in-plane technique and the needle Stimuplex D 50 mm (B. BraunMelsungen AG, Germany). Finally, after pulling up the needle, 10 ml ropivacaine 0.375% was injected into the space between the pectoralis major and minor muscles.
The paravertebral block was performed with the patient in the sitting position, at the level of thoracic vertebrae T3 and T4 under ultrasound guidance. The linear probe of the ultrasound machine General electric Logiq E (GE Healthcare, Little Chalfont, United Kingdom) was placed parallel to the spinous processes, 2.5–3 cm from the midline in the direction of the affected side. Then, under all aseptic precautions and after skin infiltration with lidocaine 1%, using an in-plane technique and the needle Stimuplex D 50 mm (B. BraunMelsungen AG, Germany), 20 ml ropivacaine 0.5% was slowly injected into the paravertebral space.
During and after performing the block, hemodynamic parameters (blood pressure, heart rate), respiration (capillary blood saturation, respiratory rate) and the patient’s subjective sensations were monitored to control the intravascular administration of the local anaesthetic or its system resorptive effects. The time for performing the blocks, including all aseptic precautions, was recorded. After the block’s procedure, the loss of tactile sensitivity in the dermatomes from T1 to T8 and according to the area of local anaesthetic distribution was assessed by pin-pricking with a sterile needle every 5 min while the patient was conscious. General anaesthesia was induced following 15–20 min with an injection of fentanyl 1–2 mg/kg and propofol 2 mg/kg. The airway patency was maintained by a laryngeal mask. The total intravenous anaesthesia was supported by a continuous infusion of propofol. Additional fentanyl 50 µg i.v. boluses were administered when we observed patient’s motor reactions or when the heart rate or systolic blood pressure has increased by more than 20% from the baseline. After awakening, the patients were transported into the ward. Ketoprofen 100 mg i.v. was administered for pain relief when pain intensity was greater than 3 points by the Numerical rating scale (NRS) or after the patient‘s request. If the pain intensity remained above 3 points after ketoprofen administration, or if the patient was subjectively unsatisfied from this analgesia, then an opioid analgesic (20 mg promedol 2%) was administered intramuscularly for pain relief.
Postoperative pain was evaluated using NRS (0–10 points; 0 = no pain and 10 = worst imaginable pain) at rest at 0, 1, 2, 6, 12, 18 and 24 hours after the surgery (if the patient slept at the scheduled time, the assessment was not conducted). There was also noted a need for ketoprofen and promedol and the time to first administration of analgesics. Postoperative nausea and vomiting were evaluated using a four-point numerical scale (1 = no nausea, 2 = mild nausea, 3 = single vomiting, 4 = multiple vomiting). All possible block-related complications were recorded, too.
The obtained data were entered into a Microsoft Excel 2007 spreadsheet (Microsoft Corporation, USA). Program “STATISTICA 10.0” (StatSoftInc., USA) was used for statistical analysis. The Shapiro-Wilk test was used to check the normality of quantitative data distribution. In the study, non-normally distributed quantitative data are presented as medians and interquartile intervals. The Mann-Whitney U-test was used to determine the significance of the differences between groups (P-value). Normally distributed quantitative data are presented as the means and the squared deviation from the mean and the intergroup differences were analyzed using the independent-sample Student’s t-test. The categorical data are presented as numbers and percentages, and the significance of the differences between groups was calculated using the Pearson’s chi-square test. The P-values < 0.05 were considered statistically significant.
Results
Sixty patients were enrolled in the study and randomized into two equal groups with no statistically significant differences in age, weight and duration of surgery. The quadrantectomy/mastectomy ratios were 14/16 in Pecs group and 13/17 in TPVB group (Tab. 1). The Peck and TPVB blocks covered 4 (3.0–5.0) and 3 (2.0–4.0) dermatomes (P = 0.0017), respectively.

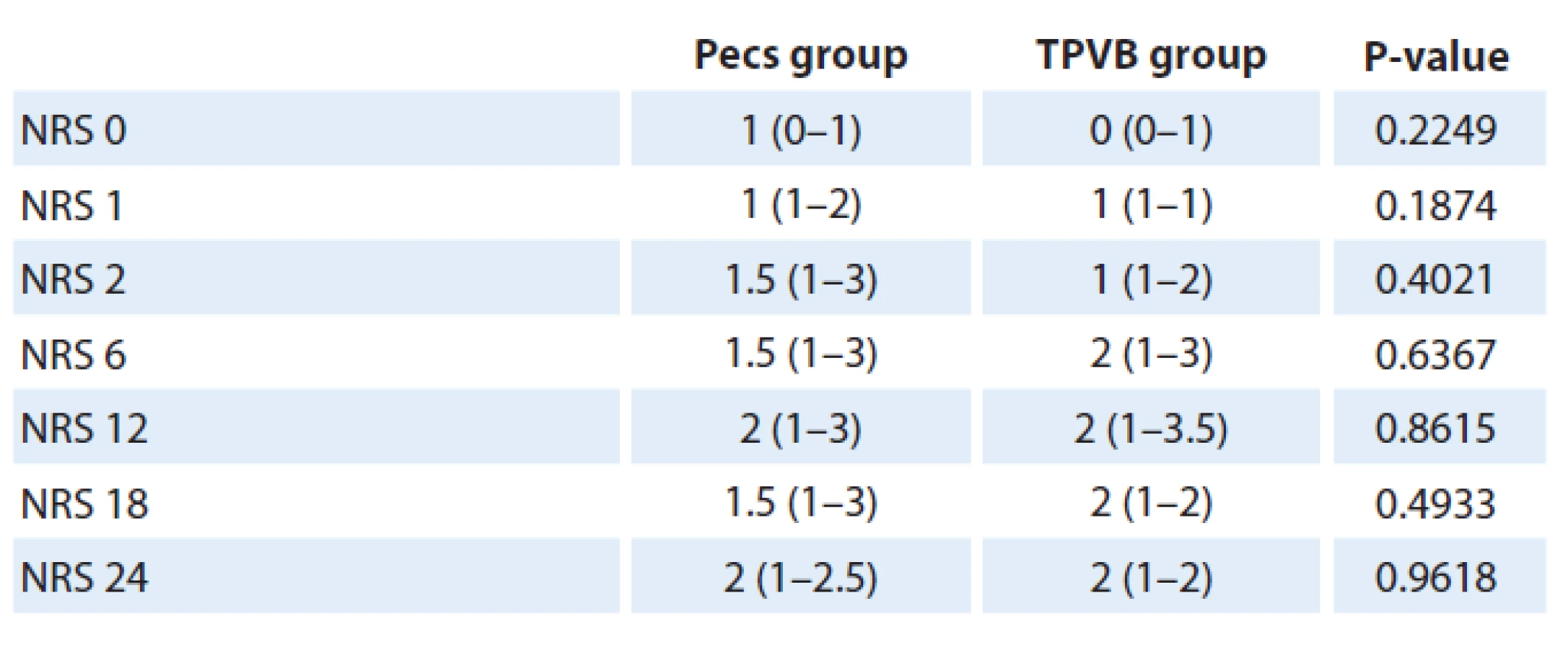
The difference in pain intensity in the postoperative period, assessed with NRS, was not statistically significant between the two groups (Tab. 2). The number of patients, who did not require any analgesia after surgery, was 10 in Pecs group and 9 in TPVB group (P = 0.793). The need for analgesia with ketoprofen was lower in Pecs group than in TPVB group, without statistical significance: 63.3 (± 66.87) and 90.0 (± 84.49) mg (P = 0.284). The number of patients who required promedol was lower in Pecs group: 6 (20%) vs. 8 (27%) (Р = 0.542). The time to first analgesic administration was longer in Pecs group compared with TPVB group but the difference was not statistically significant: 550 (400.0–600.0) and 510 (360.0–600.0) min (P = 0.5060), respectively. The rates and severity (max. score of 3 points) of nausea were higher in TPVB group than in Pecs group: 5 vs. 2 patients, respectively (P = 0.229) (Tab. 3). Two patients (6.7%) in TPVB group had perioperative complications. In the early postoperative period, one patient from TPVB group had signs of local anaesthetic system toxicity effects including convulsions and lowering of consciousness, which passed quickly after administration of 10 mg diazepam. Other patients had a significant blood pressure decrease after general anaesthesia induction and required norepinephrine infusion during surgery and in the early postoperative period. There were no complications in Pecs group.

Pecs – pectoral nerve block, TPVB – thoracic paravertebral block
Discussion
This prospective randomized study showed that pectoral nerve block type II with 30 ml ropivacaine 0.375% has a similar analgesic effect as a thoracic paravertebral block with 20 ml ropivacaine 0.5% for breast cancer surgery. The pain intensity at rest, assessed using NRS, was comparable in both groups during the first 24 hours after surgery (Tab 2). Heterogeneous data about pain intensity were obtained in previous studies. Syal et al. obtained results with significantly higher scores of the pain intensity in the pectoral nerve block group, but it should be noted that in this study, they injected 20 ml of local anaesthetic only instead of 30 ml for the block [10]. Kulhari et al reported the same pain intensity in both groups [8]. Wahba et al observed in their study lower NRS scores during the first 12 hours after the surgery in Pecs group, but during the period of 12–24 hours, the results were opposite [7]. We can note that in our study the pain intensity was lower than in similar ones, which may be related to the women’s ethnic and cultural characteristics in our region. In general, breast cancer surgery is not associated with severe postoperative pain syndrome. Gerbershagen et al have compared in their study the pain intensity during the first day after 179 types of surgical intervention. Breast cancer surgeries, such as mastectomy and quadrantectomy with axillary lymph node dissection, were performed at 146 and 160 places [18].
In our study, 10 women in Pecs group (33%) and 9 women in TPVB group (30%) did not require any analgesia during the first 24 hours. Comparing the groups, the need for opioid and non-opioid analgesics in the postoperative period was lower in Pecs group, although without a statistically significant difference. In the most currently available studies, the postoperative need for opioids (patient-controlled morphine analgesia) was higher in TPVB group, with statistical significance in three studies [7,10, 12] and without statistical significance in another one [19]. In the study of Syal et al, which compared fentanyl analgesia in the postoperative period, there was a greater need for opioids in Pecs group, but without statistical significance [10]. Although this study has the same results as most privies, we didn’t achieve a statistically significant difference in postoperative analgesics requirement in the two groups. It could be because postoperative pain intensity was generally low, and the patients require less analgesia.
The time to first rescue analgesia was longer in Pecs group and the same results were observed in other previous studies [7,8,14,19]. In previous studies, the time after surgery to the first rescue analgesia varied due to the different plans of postoperative analgesia according to the study design. In our study, we evaluated the time to first administration of either opioid or non-opioid analgesics.
The dermatomal spread after the Pecs block was significantly larger than after the paravertebral block, but it did not influence perioperative analgesia. The body’s areas spread of Pecs block and TPVB are slightly different. After the administration into the paravertebral space at Th3–Th4 level, a local anaesthetic spreads more in the caudal and less in the cranial directions [20]. It blocks the intercostal nerves, their anterior and lateral skin branches, respectively. In this case, a local anaesthetic does not block the brachial plexus and supraclavicular nerves. Kulhari et al reported that single-shot administration of 25 ml ropivacaine 0.5% caused a sensory block for a median of three segments [10], and Cheema et al reported that 15 ml bupivacaine 0.5% blocked five segments [21]. In our study, the median spread of anaesthesia was also three segments for TPVB.
After performing the Pecs block and application of a local anaesthetic injection between the pectoralis major and minor muscles and between the pectoralis minor and serratus anterior muscles, we can expect a block of 4–6 lateral cutaneous branches of the intercostal nerves and four nerves from the brachial plexus (n. thoracodorsalis, n. thoracicuslongus, nn. pectoralislateralis and medialis). An additional important factor is that a local anaesthetic moves into the axillary fossa, provides analgesia of the axillary lymph node dissection area and blocks nn. intercostobrachialis (T1–T2). This block does not anaesthetize the regions of supraclavicular nerves and anterior skin branches of intercostal nerves. Blanco et al described that the Pecs block anaesthetized four segments, which sometimes varied up to six segments [17]. Kulhari et al reported that after the injection of 15 ml of anaesthetic, the sensor block reached four segments [10]. In our study, the median spread of anaesthesia was five segments, which may be due to the local anaesthetic administration as much caudally as possible, over the 4th rib; we also used a larger volume of local anaesthetic (20 ml) than Kulhari et al. In TPVB group, the patients did not have adequate analgesia in the axillary region; thus, they required more opioid analgesics during and after major surgeries, such as mastectomy. On the other hand, the pectoral nerve block provided effective analgesia for axillary lymph node dissection and adequately anaesthetized the lateral part of the mammary gland, but it did not work when the surgeons performed incision more medially and not always worked when the incision involved lower dermatomes.
The rate and intensity of postoperative nausea were higher in TPVB group, but without statistical significance. There were two patients with nausea (assessed with 2 points) in Pecs group, and five patients in TPVB group (two of them had 3-point nausea). It can be due to the fact that the patients in TPVB group got more opioids.
As well as in previous studies [7,8, 10,19], no complications were observed after pectoral nerve blocks. Instead, in TPVB group, two patients had block-related complications (6.7%). One patient experienced a system resorptive effect of local anaesthetic, although we did not exceed the recommended safe doses for ropivacaine. The convulsions occurred after patient awakening during transportation from the operating room and were successfully treated by administration of 10 mg diazepam. Then this patient was under observation until the morning next day and she had not any health-related problems. Another patient had hypotension, which occurred after 15 min since the block performing, at the beginning of the general anaesthesia induction and required correction with small doses of norepinephrine during the surgery and the first two hours after the intervention. Tahiri et al reported in their meta-analysis that hypotension and bradycardia are the most common complications of TPVB in breast surgery, and the overall rate of complications, including pneumothorax and epidural local anaesthetic spreading, reaches up to 12% [22]. Thus, the safety profile of TPVB is better than the safety profile of Pecs
block.
The present study has several limitations. First, the TPVB was performed at one Th 3–4 level only, as in most previous researches comparing the efficacy of these two techniques [7,8,14,19], although there is evidence that the analgesic effect is better when the TPVB is performed at several levels [23]. Second, two types of breast cancer surgery were included in the study – mastectomy and quadrantectomy, both with axillary lymph node dissection. We didn’t record quadrantectomy location in Pecs group. As shown by Kim et al, postoperative opioid consumption after the Pecs block was significantly greater with tumors in the inner area of the breast than in the outer area [16]. The Pecs block produces anaesthesia of lateral cutaneous branch of intercostal nerves, medial quadrants of the breast are not anaesthetized. Third, postoperative analgesia was given “on-demand”, because we do not use patient control analgesia in wards setting. The patient control analgesia is better for a more precise estimation of opioids requires.
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
The Editorial Board declares that the manuscript met the ICMJE recommendation for biomedical papers.
Volodymyr Volodymyrovych
Martsiniv
Department of Anaesthesia and
Intensive Care
P. L. Shupyk National Medical Academy
of Postgraduate Education
3 Bratislavska str.
02156 Kyiv
Ukraine
Submitted/Obdŕžané: 18. 5. 2020
Accepted/Prijaté: 15. 6. 2020
Zdroje
The pectoral nerve block type II with ropivacaine 0.375% (Pecs block) provides efficacy which is comparable to the single-level thoracic paravertebral block (TPVB) analgesia during and after breast cancer surgery. These results allow considering this block as a good alternative to TPVB. Further larger studies are required to confirm these findings by reaching statistically significant evidence and to investigate the Pecs II effects on chronic pain development during a long-term period.
References
1. Ferlay J, Soerjomataram I, Dikshit R et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015; 136 (5): 359–386. doi: 10.1002/ijc.29210.
2. Бюлетень Національного канцер-реєстру в Україні №20. Київ, 2019. [online]. Available from: http: //www.ncru.inf.ua/publications/BULL_20/PDF_E/42-43-mol.pdf.
3. Poleshuck EL, Katz J, Andrus CH et al. Risk factors for chronic pain following breast cancer surgery: a prospective study. J Pain 2006; 7 : 626–634.
4. Rawal N. Current issues in postoperative pain management. Eur J Anaesthesiol 2016; 33 : 160–171. doi: 10.1097/EJA.0000000000000366.
5. Wu J, Buggy D, Fleischmann E et al. Thoracic paravertebral regional anesthesia improves analgesia after breast cancer surgery: a randomized controlled multicentre clinical trial. Can J Anaesth 2015; 62 (3): 241–251. doi: 10.1007/s12630-014-0285-8.
6. Das S, Bhattacharya P, Mandal MC et al. Multiple-injection thoracic paravertebral block as an alternative to general anaesthesia for elective breast surgeries: A randomised controlled trial. Indian J Anaesth 2012; 56 (1): 27–33. doi: 10.4103/0019-5049.93340.
7. Wahba SS, Kamal SM. Thoracic paravertebral block versus pectoral nerve block for analgesia after breast surgery. [online]. Available from: https: //www.sciencedirect.com/science/article/pii/S1110184913001141.
8. Kulhari S, Bharti N, Bala I et al. Efficacy of pectoral nerve block versus thoracic paravertebral block for postoperative analgesia after radical mastectomy: a randomized controlled trial. Br J Anaesth 2016; 117 : 382–386. doi: 10.1093/bja/aew223.
9. Siddeshwara A, Singariya G, Kamal M et al. Comparison of efficacy of ultrasound-guided pectoral nerve block versus thoracic paravertebral block using levobupivacaine and dexamethasone for postoperative analgesia after modified radical mastectomy: a randomized controlled trial. Saudi J Anaesth 2019; 13 (4): 325–331. doi: 10.4103/sja.SJA_25_19.
10. Syal K, Chandel A. Comparison of the post-operative analgesic effect of paravertebral block, pectoral nerve block and local infiltration in patients undergoing modified radical mastectomy: a randomised double-blind trial. Indian J Anaesth 2017; 61 (8): 643–648. doi: 10.4103/ija.IJA_81_17.
11. Hetta DF, Rezk KM. Pectoralis-serratusinterfascial plane block vs thoracic paravertebral block for unilateral radical mastectomy with axillary evacuation. J Clin Anesth 2016; 34 : 91–97. doi: 10.1016/j.jclinane.2016.04.003.
12. Versyck B, van Geffen GJ, Chin KJ. Analgesic efficacy of the Pecs II block: a systematic review and meta-analysis. Anaesthesia 2019; 74 (5): 663–673. doi: 10.1111/anae.14607.
13. Tripathy S, Mandal I, Rao PB et al. Opioid-free anesthesia for breast cancer surgery: a comparison of ultrasound guided paravertebral and pectoral nerve blocks. A randomized controlled trial. J Anaesthesiol Clin Pharmacol 2019; 35 (4): 475–480. doi: 10.4103/joacp.JOACP_
364_18.
14. Annamalai G, Durairaj AK, Kailasam KR. Pectoral nerve block versus thoracic paravertebral block – comparison of analgesic efficacy for postoperative pain relief in modified radical mastectomy surgeries. [online]. Available from: https: //www.jemds.com/data_pdf/1_ashok%20kumar-jy%2027.pdf.
15. Neethu M, Pandey RK, Sharma A et al. Pectoral nerve blocks to improve analgesia after breast cancer surgery: A prospective, randomized and controlled trial. J Clin Anesth 2018; 45 : 12–17. doi: 10.1016/j.jclinane.2017.11.
027.
16. Kim DH, Kim S, Kim CS et al. Efficacy of pectoral nerve block type II for breast-conserving surgery and sentinel lymph node biopsy: a prospective randomized controlled study. Pain Res Manag 2018; 2018 : 4315931. doi: 10.1155/2018/4315931.
17. Blanco R, Fajardo M, Parras MT. Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim 2012; 59 : 470–475. doi: 10.1016/j.redar.2012.07.003.
18. Gerbershagen HJ, Aduckathil S, van Wijck AJ et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013; 118 (4): 934–944. doi: 10.1097/ALN.0b013e31828866b3.
19. El-Sheikh SM, Fouad A, Bashandy GN et al. Ultrasound guided modified pectoral nerves block versus thoracic paravertebral block for perioperative analgesia in major breast surgery. Medical Journal of Cairo University 2016; 84 : 189–195.
20. Marhofer D, Marhofer P, Kettner SC et al. Magnetic resonance imaging analysis of the spread of local anesthetic solution after ultrasound-guided lateral thoracic paravertebral blockade. Anesthesiology 2013; 118 (5): 1106–1112. doi: 10.1097/ALN.0b013e318289465f.
21. Cheema SPS, Ilsley D, Richardson J et al. A thermographic study of paravertebral analgesia. Anaesthesia1995; 50 : 118–121. doi: 10.1111/j.1365-2044.1995.tb15092.x.
22. Tahiri Y, Tran DQ, Bouteaud J et al. General anaesthesia versus thoracic paravertebral block for breast surgery: a meta-analysis. J Plast Reconstr Aesthet Surg 2011; 64 (10): 1261–1269. doi: 10.1016/j.bjps.2011.03.025.
23. Kasimahanti R, Arora S, Bhatia N et al. Ultrasound-guided single - vs double-level thoracic paravertebral block for postoperative analgesia in total mastectomy with axillary clearance. J Clin Anesth 2016; 33 : 414–421. doi: 10.1016/j.jclinane.2016.01.027.
Štítky
Detská onkológia Chirurgia všeobecná OnkológiaČlánok vyšiel v časopise
Klinická onkologie

2020 Číslo 4
- Brno opět přivítá onkology a nelékařské zdravotnické pracovníky
- I „pouhé“ doporučení znamená velkou pomoc. Nasměrujte své pacienty pod křídla Dobrých andělů
- Realita liečby bolesti v paliatívnej starostlivosti v Nemecku
- MUDr. Lenka Klimešová: Multiodborová vizita je kľúč k efektívnejšej perioperačnej liečbe chronickej bolesti
- Fixní kombinace tramadol/paracetamol je doporučenou volbou v léčbě chronické bolesti v ordinaci praktického lékaře
Najčítanejšie v tomto čísle
- Zhubné nádory krčka maternice v gravidite
- Integrovaná diagnostika difúzních gliomů
- Atypický průběh typického karcinoidu plic
- Nemoc těžkých řetězců imunoglobulinu gama