
Prevalence and hormonal profiling of secondary amenorrheic patients presenting to a fertility clinic – an observational study
Prevalence a hormonální profilování sekundárních amenoreických pacientek dostavujících se na kliniku plodnosti – observační studie
Cíl: Amenorea je menstruační porucha, která může vzniknout v důsledku hormonální dysfunkce osy hypothalamus-hypofýza-gonády. O nejčastějších příčinách sekundární amenorey v Pákistánu existuje jen omezené množství údajů. Cílem této studie bylo proto posoudit různé kauzativní faktory spolu s hormonálním profilem u pacientek se sekundární amenoreou. Pacientky a metody: Tato průřezová studie byla provedena na různých klinikách pro léčbu neplodnosti v Abbottabadu. Pacientky se sekundární amenoreou byly zařazeny pomocí metody no-probability samplingu. Data týkající se demografických a dalších klinických proměnných byla shromážděna prostřednictvím formuláře pro sběr dat. Sérové hladiny progesteronu, estradiolu, luteinizačního hormonu, folikuly stimulujícího hormonu a prolaktinu byly stanoveny pomocí komerčně dostupných sad pro enzymově vázanou imunosorbentní analýzu. Tato studie byla provedena na 126 pacientkách s průměrným věkem 28,5 ± 7,8 let. Výsledky: Amenorea související s léky byla pozorována u 14,3 % pacientek. Amenorea vyvolaná hyperprolaktinemií byla pozorována u 31,7 % a 54 % pacientek bylo s neznámou etiologií. Z pacientek s amenoreou vyvolanou léky užívalo 38,9 % perorální antikoncepci, 27,8 % omeprazol a 33,3 % jiné léky. Bolest hlavy (79,4 %) a únava (78,6 %) byly hlavními příznaky hlášenými u amenoreických žen, zatímco vypadávání vlasů bylo hlášeno u 65,9 % pacientek. Ztráta libida a hirsutizmus byly pozorovány u 45,2 %, resp. 42,9 % pacientek. Bolest prsou a vaginální suchost se vyskytly u 35,7 %, resp. 23,8 % pacientek. Závěr: Současná studie ukázala, že hyperprolaktinemie je nejčastější příčinou sekundární amenorey, následované amenoreou vyvolanou léky, což je třeba vzít v úvahu při klinické léčbě hormonální nerovnováhy a následné amenorey.
Klíčová slova:
Hormones – amenorrhea – drug-induced abnormalities – hyperprolactinemia
Authors:
Nayab Iqbal; Muhammad Ashfaq
![]() ; Qasim Khan
; Qasim Khan
![]() ; Syed Mobasher Ali Abid; Muhammad Junaid Hassan Sharif
; Syed Mobasher Ali Abid; Muhammad Junaid Hassan Sharif
![]() ; Yasser Msa Alkahraman
; Yasser Msa Alkahraman
![]()
Authors place of work:
Department of Pharmacy, COMSATS University Islamabad, Abbottabad Campus, Abbottabad, Pakistan
Published in the journal:
Ceska Gynekol 2025; 90(5): 374-379
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg2025374
Summary
Objective: Amenorrhea is a menstrual disorder than can arise as a result of hormonal dysfunction of the hypothalamic-pituitary--gonadal axis. There is limited data on the most common causes of secondary amenorrhea in Pakistan. Therefore, this study aimed to assess various causative factors along with hormone profiling in patients with secondary amenorrhea. Patients and methods: The present cross-sectional study was conducted in different fertility clinics of Abbottabad. Patients with secondary amenorrhea were included by a non-probability sampling technique. Data related to demographic and other clinical variables were collected via a data collection form. Serum progesterone, estradiol, luteinizing hormone, follicle stimulating hormone, and prolactin were determined using commercially available enzyme-linked immunosorbent assay kits. This study was conducted on 126 patients with a mean age of 28.5 ± 7.8 years. Results: Drug-related amenorrhea was observed in 14.3% of patients. Hyperprolactinemia-induced amenorrhea was observed in 31.7% and in 54% of patients with unknown etiology. Of the patients with drug-induced amenorrhea, 38.9% used oral contraceptives, 27.8% used omeprazole, and 33.3% used other drugs. Headache (79.4%) and fatigue (78.6%) were the main symptoms reported in amenorrheic women, while hair loss was reported in 65.9% of patients. Both loss of libido and hirsutism were observed in 45.2% and 42.9% of patients, resp. Breast pain and vaginal dryness occurred in 35.7% and 23.8% of patients, resp. Conclusion: The current study showed that hyperprolactinemia is the most common cause of secondary amenorrhea followed by drug-induced amenorrhea, which must be considered in the clinical management of hormonal imbalances and subsequent amenorrhea.
Keywords:
Hormones – amenorrhea – hyperprolactinemia – drug-induced abnormalities – amenorea – abnormality vyvolané léky – hyperprolaktinemie – hormony
Introduction
Amenorrhea is one of the most important and challenging endocrine diseases in gynecology [1]. Amenorrhea can be a temporary, intermittent, or permanent disorder caused by hypothalamic, pituitary, ovarian, uterine, or vaginal malfunction [2]. Amenorrhea is classified into primary and secondary amenorrhea. Primary amenorrhea is defined as the failure to reach menarche and the absence of menses by the age of 14 to 6 in the lack of secondary sexual characteristics growth or development [3]. Primary amenorrhea affects 3% of women around the world [4]. There are many causes of primary amenorrhea such as central regulatory diseases including pituitary disorders, hypothalamic diseases, pituitary tumors, androgen insensitivity, congenital gonadotropin-releasing hormone (GnRH) insufficiency, and Kallmann syndrome [5,6].
Secondary amenorrhea is the stoppage of preceding regular periods for 3 months or preceding irregular periods for 6 months [7]. An imbalance in the hypothalamic-pituitary-adrenal axis is nearly half of all occurrences of secondary amenorrhoea [8]. The prevalence of secondary amenorrhea is 5–7% [9]. For women of childbearing age, the most common physiological causes of absent menstrual periods are pregnancy and lactation [10]. Whereas, pathological causes include hypothalamic amenorrhea, hyperprolactinemia, thyroid dysfunction, primary ovarian insufficiency, and polycystic ovary syndrome [11,12]. Certain drugs such as H2 receptor antagonists, antidepressants, antipsychotics, antiepileptics, opioids and heroin, contraceptives, antihypertensive, and proton pump inhibitors (PPIs) may also lead to menstrual irregularities [13–15].
It is evident from the literature that the number of women experiencing menstural irregularities including secondary ammenohea during reproductive age has significantly increased in developing countries [16]. It is also revealed that there is a limited number of studies regarding the prevalence of functional secondary amenorrhea, its associated factors, and infertility induced by hormonal imbalances [17]. However, data regarding secondary amenorrhea and its specific causes such as various medications is currently lacking in Pakistan.
Therefore this study aimed to:
identify different categories of secondary amenorrhea;
perform analysis of different reproductive hormones;
compare levels of different reproductive hormones among amenorrhea patients on medications such as contraceptives, PPIs, and other medications.
Method and materials
Study design, time frame, and ethical approval
This cross-sectional study was carried out at Medical Teaching Institute (MTI), Ayub Teaching Hospital (ATH), and Dr. Ruqqiya’s maternity clinic in Abbottabad from 1st November 2020 to 31st January 2021. 126 cases of secondary amenorrhea between ≥ 14 and > 40 years of age were recruited after the ethical approval from the ethical committee of Department of Pharmacy, COMSATS University Islamabad, Abbottabad vide letter number (PHM.Eth/CF-M10/17-009-3).
Sample size
For calculation of sample size following formula was used in the prevalence study [18].

Inclusion and exclusion criteria
Patients with ≥14 years of age diagnosed with secondary amenorrhea were included. Patients with primary amenorrhea were excluded from this study.
Procedure
Each patient in the current sample when came to maternity clinics was interviewed with a set of queries regarding details of demographic, clinical characteristics, previous endocrine diseases, previous long-term medications, and menstrual patterns in a self-created data collection form.
After taking thorough histories from the patients, 5–10 mL blood sample was taken via intravenous (I/V) route from each individual [19]. The obtained blood was transferred from the syringe to the gel tube and was inverted 5–6-times. Then the blood was left at room temperature for (20) minutes, after which the serum was separated using a centrifuge at a speed of 3,000 revolutions per minute (rpm) for 10 minutes, after which the serum was withdrawn using a micropipette. The separated serum was placed in Eppendorf and then stored in a deep freezer to preserve it at low temperatures until the required tests are carried out.
Measuring levels of the different reproductive hormones in secondary amenorrhea patients by using ELISA kits
The levels of different reproductive hormones were measured by following the steps according to the manufacturer’s instructions for the Elisa device.
Statistical analysis
Descriptive statistics were used to calculate frequencies and percentages of study variables. Study variables were evaluated by a non-parametric test, the Kruskal-Wallis test, for comparison among different classes of medications used with respect to changes caused by reproductive hormones levels. P ≤ 0.05 was considered statistically significant. Statistical analyses were carried out using IBM Statistical Package for Social Sciences version 20 (IBM SPSS v-20) used for data analysis.
Result
A total of 126 patients presenting with secondary amenorrhea were included in the study. The mean age of the study population was 28.46 ± 7.79. Tab. 1 summarizes frequencies and percentages of sociodemographic characteristics. The majority of patients (53.2%) were between 21–30 years, followed by 31–40 years (22.2%), ≤ 20 years (15.9%), and > 40 years (8.7%). Among the study population, most of the patients were married (88.9%). According to the occupational status of the patients, the majority (83.3%) were housewives, followed by students (11.9%), teachers (3.2%), and health workers (1.6%). The previous history was taken from the amenorrhea patients. Most (91.3%) were shown to have no family history of amenorrhea, whereas there was a previous history of amenorrhea in mother (4%) and sister (5.6%). According to body mass index (BMI) categories, 43.7% of patients were overweight followed by 34.9% with normal BMI and 13.5% obese, and 7.9% underweight patients. Various comorbid diseases include polycystic ovary syndrome (14.3%), hypertension (13.5%), and diabetes mellitus (4.8%) (Tab. 1).
The clinical characteristics of patients are recorded in Tab. 2. The most frequent symptoms include, headache (79.4%), fatigue (78.6%), generalized body pain (73.8%), anxiety (67.5%), hair loss (65.9%), weight gain (63.5%), abdominal pain (57.9%), mood swings (55.6%), irritability (53.2%), nausea (50.8%), acne (48.4%), anorexia (46.8%), palpitations (46.8%), hot flushes (46.8%), loss of libido (46.8%), hirsutism (42.9%), pain in breast (35.7%), sleep disturbance (32.5%), visual disturbance (27%) constipation (27%), difficulty in concentration (26.2%), vaginal dryness (23.8%), weight loss (23%), breast enlargement (22.2%), night sweats (16.7%), bladder control problem (15.1%), psychotic disorder (9.5%) and galactorrhoea (7.1%) (Tab. 2).
The frequencies of different categories of secondary amenorrhea are illustrated in Fig. 1. Among 126 amenorrhoeic patients, causative factors include hyperprolactinemia (31.7%), medications (14.3%), and miscellaneous causes irrespective of either drugs or hyperprolactinemia (54%). It was observed that in drug-induced amenorrhea, the majority of patients (38.9%) were on oral contraceptives followed by other drugs such as H2 receptor antagonists, antidepressants, antiepileptic and antihypertensive agents (33.3%), and omeprazole (27.8%) (Fig. 1).
Tab. 3 demonstrates comparisons between study variables such as different classes of medications and their corresponding effects on hormonal levels by applying the Kruskal Wallis H test. A statistically significant difference (P = 0.04) was observed among contraceptives, PPIs, and other drugs in amenorrhoeic women with respect to estradiol levels. Whereas there was no statistically significant difference among contraceptives, PPIs and other drugs with respect to other hormones such as total prolactin (P = 0.3), monomeric prolactin (P = 0.3), progesterone (P = 0.2), follicle-stimulating hormone (P = 0.6) and luteinizing hormone (P = 0.1). Pairwise comparison analysis for estradiol shows there was a statistical difference between the mean rank of PPIs and other drugs while PPIs and contraceptives, contraceptives, and other drugs show no significant differences between mean ranks of these groups (Tab. 3).



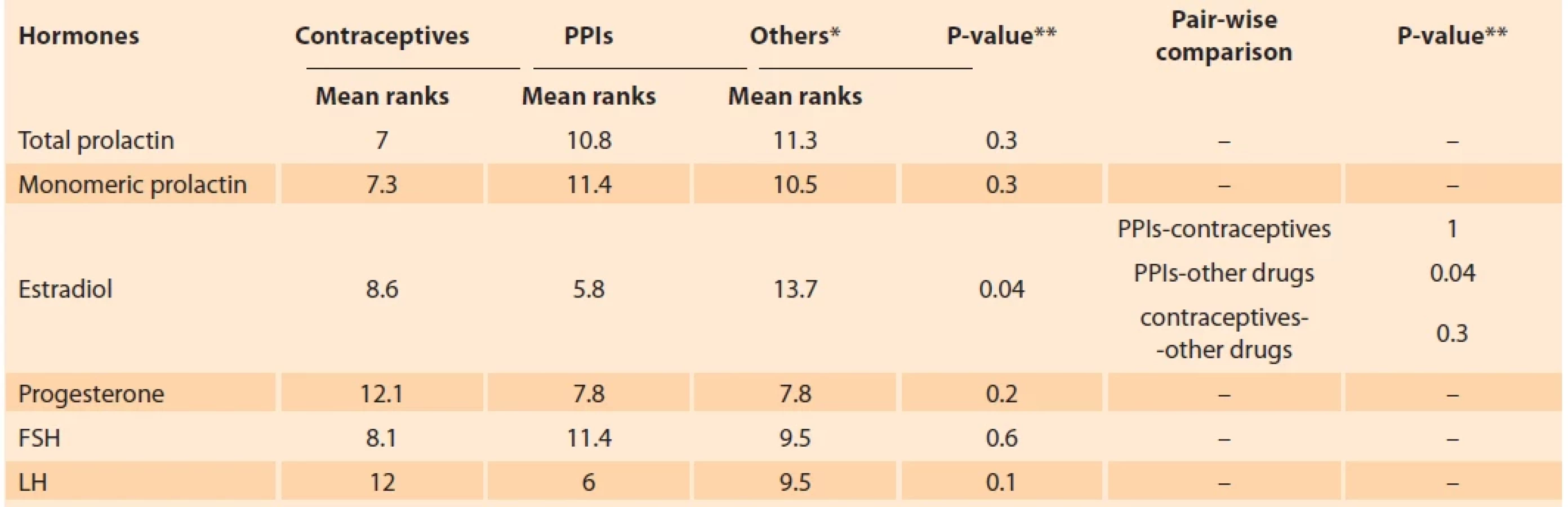
**P-value ≤ 0.05 was considered statistically signifi cant.
FSH – follicle-stimulating hormone/folikulostimulační hormon, LH – luteinizing hormone/luteinizační hormon, PPIs – proton pump inhibitors/
inhibitory protonové pumpy
Discussion
This study was carried out to assess the hormonal profile of women within drug-induced secondary amenorrhea in different fertility clinics of Abbottabad. This is the first study conducted by infertility clinics in Abbottabad. The majority of amenorrhoeic cases were either drug or hyperprolactinemia induced whereas, causes other than medications and hyperprolactinemia were also identified. The prevalence of hyperprolactinemia was considerably higher (31.7%) in our study as compared with previous studies where its prevalence was 9–17% [20]. The underlying causes for such a higher prevalence of hyperprolactinemia may include various medications or other diseases. Other potentially contributing factors of amenorrhea in our study population include poly cystic ovary syndrome (PCOS), thyroid disorders, diabetes mellitus, fibroids, kidney infections, cardiac diseases, hypertension and gastrointestinal disturbances.
The current study showed a higher prevalence of drug induced amenorrhea patients was 14.3% as compared with previous studies which showed that the prevalence due to medications was 9% [21]. Among drug-induced cases, the majority were taking antihypertensive, antidepressants, antipsychotics, and H2 receptor antagonists. These medications mainly disturb the menstrual cycle by interfering with the hypothalamic-pituitary axis and cause amenorrhea. The study findings warrant caution regarding use of these medications to avoid subsequent hormonal irregularities.
Our study described that participants using antidepressants were more prone to secondary amenorrhea. The most frequently used antidepressant drugs in our study include fluoxetine, fluvoxamine, escitalopram, and amitriptyline. The literature shows that escitalopram causes amenorrhea by suppressing hypothalamic gonadotropin-releasing hormone due to elevated levels of prolactin and thus decreasing the production of gonadotropins such as luteinizing hormone and follicle-stimulating hormone [22]. Antipsychotic-induced amenorrhea is a common but neglected adverse effect in clinical practice. In this study, risperidone was found to be associated with an increased serum level of prolactin after its use for more than 2 years. Another study also reported a similar pattern that amenorrhea was obvious in patients who were exposed to antipsychotics for more than 2 years [8].
Moreover, PPIs are included among the agents associated with hyperprolactinemia. Our study demonstrated a considerable use of PPIs which may lead to hyperprolactinemia and subsequent menstrual irregularities. It is established from the literature that proton pump inhibitors used either alone or in combination with prokinetics cause hyperprolactinemia [23]. Another study showed that PPIs can trigger hyperprolactinemia resulting in Amenorrhea and cyclic disturbances through hormonal abnormalities [15].
The study findings demonstrate that the use of contraceptives was quite common among amenorrhoeic patients. The literature shows that the primary contraceptive mechanism of the combination OCP is to prevent ovulation by inhibiting gonadotropin secretion at both the level of the pituitary gland and the hypothalamus [24]. Another study showed that hormonal contraceptives (HCs) are responsible for a decrease of circulating androgen levels as well as serum levels of estradiol and progesterone from the ovary and the inhibition of oxytocin functioning [25]. It is evident from the study findings that secondary amenorrhea can be caused by a myriad of factors. However, this can be reduced by thorough clinical assessment of patients before selecting drug therapy, promoting rational use of medications and addressing other contributing factors such as hormonal irregularities and diseases.
Conclusion
The current study demonstrated that hyperprolactinemia, various medications and other predisposing factors are responsible for secondary amenorrhea. There is a need to address these issues to avoid hormonal irregularities and subsequent amenorrhea. Appropriate measures such as careful selection of pharmacotherapy is also required to avoid harmful consequences in clinical practice.
Zdroje
1. Gordon CM, Ackerman KE, Berga SL et al. Functional hypothalamic amenorrhea: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2017; 102 (5): 1413–1439. doi: 10.1210/jc.2017-00131.
2. Reza Radjabi A, Keefe DL. Amenorrhea. Evidence-based obstetrics and gynecology. USA, NJ: John Wiley & Sons 2019 : 108–115. doi: 10.1002/9781119072980.ch11.
3. Samal R, Habeebullah S. Primary amenorrhea: a clinical review. Int J Reprod Contracept Obstet Gynecol 2017; 6 (11): 4748–4753. doi: 10.18203/2320-1770.ijrcog20174981.
4. Rajitha V, Rekha G, Manjunath KY et al. Role of hormones, body mass index & fasting blood glucose levels in amenorrhea cases. Int J Health Sci Res 2017; 7 (6): 108–115.
5. Khan NT, Jameel N. Amenorrhea – an abnormal cessation of normal menstrual cycle. Clin J Obstet Gynecol 2020; 3 : 033–036. doi: 10.29328/journal.cjog.1001046.
6. Wilson GR, Haddad JE, Haddad CJ. Amenorrhea: common causes and evaluation. Compr Ther 2005; 31 (4): 270–278. doi: 10.1385/ comp: 31 : 4: 270.
7. Yoon JY, Cheon CK. Evaluation and management of amenorrhea related to congenital sex hormonal disorders. Ann Pediatr Endocrinol Metab 2019; 24 (3): 149–157. doi: 10.6065/apem.2019.24.3.149.
8. Savarimuthu MK, Bhaskar S, Alexander AM et al. A cross sectional study on antipsychotic induced amenorrhoea in women attending a tertiary care centre in South India. Int J Res Med Sci 2019; 7 (6): 2067–2071. doi: 10.18203/2320-6012.ijrms20192123.
9. Butnariu L, Covic M, Ivanov I et al. Clinical and cytogenetic correlation in primary and secondary amenorrhea : retrospective study on 531 patients. Rev Rom Med Lab 2011; 19 (2): 149–160.
10. Klein DA, Poth MA. Amenorrhea: an approach to diagnosis and management. Am Fam Physician 2013; 87 (11): 781–788.
11. Puscheck EE. Secondary amenorrhea. Clinical gynecology. 2nd ed. Cambridge: Cambridge university press 2015 : 942–957.
12. Štelcl M, Vrublovský P, Machač Š. Prolactin and alteration of fertility. Ceska Gynekol 2018; 83 (3): 232–235.
13. Lania A, Gianotti L, Gagliardi I et al. Functional hypothalamic and drug-induced amenorrhea: an overview. J Endocrinol Invest 2019; 42 (9): 1001–1010. doi: 10.1007/s40618-019 - 01013-w.
14. Torre DL, Falorni A. Pharmacological causes of hyperprolactinemia. Ther Clin Risk Manag 2007; 3 (5): 929–951.
15. Ashfaq M, Khan Q, Haroon MZ et al. Effects of long-term proton pump inhibitor use on sexual hormones and sexual and reproductive health in female patients. Endocrine 2024; 83 (2): 494–501. doi: 10.1007/s12020-023 - 03572-8.
16. Harlow SD, Campbell OM. Epidemiology of menstrual disorders in developing countries: a systematic review. BJOG 2004; 111 (1): 6–16. doi: 10.1111/j.1471-0528.2004.00012.x.
17. Kafeel H, Rukh R, Zubair A et al. Prevalence and factors associated with functional secondary amenorrhea. Int J Pharm 2014; 4 : 16–21.
18. Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench 2013; 6 (1): 14–17.
19. World Health Organization. Best practices in phlebotomy. WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy. 2010 [online]. Available from: https: //www.who.int/ publications/i/item/9789241599221.
20. Jain U, Jain D, Jain A. Pattern of clinical presentation of hyperplolactinemia among infertile patients. Paripex Indian J Res 2021; 10 (7): 1–13. doi: 10.36106/paripex/3607292.
21. Priyanka S, Anubha V, Kumar SR. Secondary amenorrhea: causes, management and outcome using algorithmic approach. IOSR J Dental Med Sci 2017; 16 (5): 87–91. doi: 10.9790/0853-1605128791.
22. Selvaraj V, Hour S, Gunasekar P et al. Escitalopram-induced amenorrhea and false positive urine pregnancy test. Korean J Fam Med 2017; 38 (1): 40–42. doi: 10.4082/kjfm.2017. 38.1.40.
23. Venkatanarasu A, Boddula R, Basavaraju S et al. Drug induced hyperprolactinemia. J Endocrine Soc 2021; 5 (Suppl 1): A626–A627. doi: 10.1210/jendso/bvab048.1277.
24. Wright KP, Johnson JV. Evaluation of extended and continuous use oral contraceptives. Ther Clin Risk Manag 2008; 4 (5): 905–911. doi: 10.2147/tcrm.s2143.
25. Casado-Espada NM, de Alarcón R, de la Iglesia-Larrad JI et al. Hormonal contraceptives, female sexual dysfunction, and managing strategies: a review. J Clin Med 2019; 8 (6): 908. doi: 10.3390/jcm8060908.
ORCID of authors
M. Ashfaq 0000-0002-0245-0051
Q. Khan 0000-0001-6428-4434
M. J. H. Sharif 0000-0003-2301-8134
Y. MSA Alkahraman 0009-0009-2828-9823
Submitted/Doručeno: 17. 4. 2025
Accepted/Přijato: 30. 6. 2025
Yasser MSA Alkahraman, PhD
Department of Pharmacy
COMSATS University Islamabad
Abbottabad Campus
University road, Tobe camp Abbottabad, Pakistan
yasser@cuiatd.edu.pk
Štítky
Detská gynekológia Gynekológia a pôrodníctvo Reprodukčná medicínaČlánok vyšiel v časopise
Česká gynekologie

2025 Číslo 5
- I „pouhé“ doporučení znamená velkou pomoc. Nasměrujte své pacienty pod křídla Dobrých andělů
- Gynekologické potíže pomáhá účinně zvládat benzydamin
- Mýty a fakta ohledně doporučení v těhotenství
- Jak podpořit využití železa organismem bez nežádoucích účinků
- Gynekologové a odborníci na reprodukční medicínu se sejdou na prvním virtuálním summitu
Najčítanejšie v tomto čísle
- Vaginální fisting a riziko anogenitálního poranění
- Placentární insuficience a pozdní růstová restrikce ve skupině plodů s adekvátní velikostí pro dané gestační stáří
- Results of the Endometriosis Health Profile-30 questionnaire in women aged 18– 30 years in the Czech Republic
- Prevalence and hormonal profiling of secondary amenorrheic patients presenting to a fertility clinic – an observational study