
Postoje sester a studentů ošetřovatelství k očkování proti covid-19 – přehled
Postoje sester a studentů ošetřovatelství k očkování proti covid-19 – přehled
Cíl: Téma očkování zdravotníků proti covid-19 je předmětem diskusí především v případě zdravotních sester. Primární otázkou pro tento literární přehled bylo: “Jaké jsou postoje sester vůči očkování proti covid-19 ve srovnání s ostatními typy zdravotnických profesí?” Druhou otázkou bylo, jaký je podíl sester, které se chystají nechat se očkovat a dále co sestrám v očkování brání, a naopak co jim pomůže při rozhodování nechat se očkovat.
Metody: Pro přehledovou práci byl použit formát PRISMA-ScR pro přehledy typu scoping review s ohledem na novou oblast vakcín proti covid-19. V databázích (PubMed/MEDLINE, PROquest and EBSCO) byly vyhledány původní studie ze všech zemí světa, publikované v anglickém jazyce před 20. březnem 2022.
Ochota nechat se očkovat byla hodnocena v jedné kategorii společně pro zdravotní sestry a studenty ošetřovatelství, zatímco ve druhé kategorii byli ostatní zdravotničtí pracovníci. Vývoj postojů sester k očkování v čase ve vztahu k postoji ostatních zdravotníků byl vyhodnocen post hoc.
Faktory spojené s ochotou nechat se očkovat proti covid-19 byly rozděleny podle kategorií WHO (kontextuální vlivy, individuální/ skupinové vlivy a otázky specifické pro očkování/danou vakcínu) a jsou shrnuty v narativním přehledu.
Výsledky: Celkem bylo do přehledu zařazeno 58 studií, které všechny měly průřezové dotazníkové uspořádání, a kterých se zúčastnilo 95 418 zdravotníků (včetně 33 130 sester a 7 391 studentů ošetřovatelství) v 44 zemích Evropy, Ameriky, Afriky a Asie. Hlavní kontextuální faktory, které v hodnocených studiích zvyšovaly ochotu nechat se očkovat, byly důvěra ve vědu, důvěra v lékaře, v odborníky a ve vládní instituce, zatímco altruismus a kolektivní ochrana nebo ochrana ohrožených osob v domácnosti dotazovaných zdravotníků byly zmíněny pouze v malém počtu studií. V počátečních obdobích očkování, tedy před uvedením vakcín do praxe, uváděly sestry nižší ochotu nechat se očkovat než lékaři a ostatní zdravotníci a tento rozdíl mezi zdravotnickými profesemi v čase klesal (p = 0,022). Ochota nechat se očkovat se zvyšovala s rostoucím věkem (n = 25 studií), vyšším stupněm dosaženého vzdělání (n = 7), vyšším počtem let v klinické praxi (n = 4) a byla vyšší u mužů než u žen (n = 23). Pouze v malém poštu studií uváděli zdravotníci jako důvod pro očkování pociťované vysoké osobní riziko těžkého průběhu infekce covid-19 (n = 14) nebo práci na covidových jednotkách (n = 5). Mezi hlavní faktory spojené s vakcinací či vakcínou, které zvyšovaly ochotu nechat se očkovat, patřily důvěra ve vakcínu a v její účinnost a bezpečnost, celkový pozitivní vztah k očkování a především absolvované očkování proti chřipce v předchozích letech (n = 21 studií). Významným faktorem spojeným s vyšší ochotou nechat se očkovat patřila “vakcinační gramotnost”, “pochopení vakcinace”, “znalosti o vakcinaci” případně “pochopení výhod a nevýhod očkování” (n = 17 studií).
Závěry: Zdravotní sestry byly zpočátku méně ochotné nechat se očkovat proti covid-19 než ostatní zdravotníci, ale tento rozdíl postupem času vymizel. Podobně váhavý vyčkávací postoj sester k očkování se projevuje i v údajích realizovaného očkování zdravotníků proti covid-19, které registruje Ústav zdravotnických informací a statistiky ČR. Důvěra ve vědecké instituce a výrobce vakcín zvyšuje ochotu nechat se očkovat. Tato ochota také roste s rostoucím věkem, vyšším stupněm vzdělání, delší dobou klinické praxe a také je vyšší u mužů. Mezi nezávislé, zevní intervencí potenciálně ovlivnitelné faktory spojené s vyšší ochotou nechat se očkovat patří vakcinační gramotnost a účast v jiném očkovacím programu, především v případě očkování proti sezonní chřipce.
Klíčová slova:
zdravotníci – očkování – COVID-19 – postoje – ochota nechat se očkovat – váhavost k očkování – odmítání očkování – zdravotní sestry
Authors:
A. Chrdle 1,2,3; S. Bártlová 1; I. Chloubová 1
Authors place of work:
University of South Bohemia in České Budějovice, Faculty of Health and Social Sciences, Institute of Nursing, Midwifery and, Emergency Care, České Budějovice, Czechia
1; Infectious Disease Department, České Budějovice Hospital, České Budějovice, Czechia
2; Tropical and Infectious Diseases Unit, Royal Liverpool University Hospital, Liverpool, UK
3
Published in the journal:
Epidemiol. Mikrobiol. Imunol. 72, 2023, č. 1, s. 25-39
Category:
Souhrnné sdělení
Summary
Aim: There is a discussion about COVID-19 vaccination rates among healthcare workers (HCW), especially nurses. The primary question for this review was: “What are the attitudes of nurses, compared to other HCW, towards COVID-19 vaccination?” The secondary questions included the proportion of nurses with intention to get vaccinated, what prevents the nurses from accepting the vaccine and what enables them to accept the vaccine.
Methods: The PRISMA-ScR format for scoping reviews was chosen to respect the novelty of COVID-19 vaccines. Database search (PubMed/MEDLINE, PROquest and EBSCO) was performed for original studies in English language, from all geographies, with most recent search on March 20, 2022.
Vaccination acceptance rates were charted for nurses and nursing students in one category, and HCW other than nurses in the other category. The evolution in time of the nurses attitude to vaccine acceptance relative to that of HCW other than nurses was charted post hoc.
The factors associated with COVID-19 vaccination intention according to the WHO categories (contextual influences, individual/ group influences, and vaccine/vaccination specific issues) were reviewed as narrative summary.
Results: Total 58 eligible studies were selected, all with cross-sectional study design, including 95418 healthcare workers of whom 33130 were nurses and 7391 were nursing students, from 44 countries in Europe, Americas, Africa and Asia. Trust in science, in doctors, in experts and in governments were the main contextual factors increasing vaccination acceptance mentioned in the studies, while altruism and collective protection, or protecting a person at risk at home was mentioned only few times.
The nurses were less likely to accept vaccination compared to doctors and other HCWs at the onset, eg. before vaccine rollout, and this difference decreased with time (p = 0.022). Being older (n = 25 studies), being male (n = 23), having higher degree of education (n = 7), and having more years of clinical practice (n = 4) were associated with higher vaccination acceptance. Percieved individual risk of having severe COVID-19 (n = 14) or working in a COVID-19 dedicated units (n = 5) was mentioned in a minority of studies. The main vaccine-releated factors associated with higher vaccination intention were trust in the vaccine and its efficacy and safety, general vaccinatoin acceptance and specifically having had influenza vaccination in previous years (n = 21 studies). A significant factor associated with higher vaccine acceptance was high “vaccine knowledge”, “vaccine literacy”, „understanding the vaccine” or “understanding benefits and barriers of vaccination” (n = 17 studies).
Conclusions: Nurses have been more hesitant to accept COVID-19 vaccination than other healthcare professions at the beginning, but with time this difference disappeared. This general nurse attitude of wait-and-see reported in the studies corresponds with real-life data from practicing healthcare workers as reported by the Czech Institute of Health Information and Statistics on vaccination against COVID-19.
Trust in scientific structures and vaccine makers increases the vaccine acceptance. The acceptance increases also with higher age, increasing level of education, longer clinical experience, and also with being a male. Vaccine literacy and having participated in previous vaccination programmes, especially influenza vaccine, were identified as independent modifiable factors increasing vaccination acceptance.
Keywords:
vaccination – healthcare workers – Nurses – COVID-19 – attitude – acceptance – hesitancy – refusal
INTRODUCTION
Nursing profession has a high moral position in the community and public when it comes to acceptance or endorsement of health interventions including vaccination [1]. The nurses are the highest in numbers amongst healthcare workforce, and therefore their informal influence is far reaching. Apart from that, nurses are most frequently of the healthcare professions in extended close contacts with patients and therefore, are inherently the largest population that can be associated with spread of airborne diseases in healthcare settings (in both directions, they can get infected as well as they can spread the infection) [2]. Historically, acceptance of influenza vaccine, including pandemic influenza vaccine, varied amongst nurses [3]. In covid-19 scenario, there are new factors compared to previous viral respiratory outbreaks. These include the novelty of the virus and its behaviour (variably virulent and far more contagious compared to the 2003 SARS-CoV-1 or 2012 MERS coronaviruses) [4], rapid development and rollout of innovative vaccines [5], and major change in interhuman communication patterns [6, 7].
More than one year after COVID-19 vaccination rollout across the healthcare systems, the vaccine coverage in healthcare workers appeared suboptimal [8].
We have reviewed the attitudes of nurses to covid vaccination and the driving forces behind covid-19 vaccine acceptance or hesitancy across geographical areas and cultures compared to other categories of HCW. The format of scoping review was chosen as this is a new disease and a novel situation and therefore we perceived the need to map the literature on this topic to identify key concepts, gaps in the research, and types and sources of evidence to refine the future research question and objectives. We have followed the PRISMA-ScR scoping review format [9].
The main research foreground question was “What are the attitudes of nurses, compared to other HCW, towards COVID-19 vaccination?” The secondary questions were what are the proportion of nurses with intention to get vaccinated, what prevents the nurses from accepting the vaccine and what enables them to accept the vaccine. As the literature mostly includes nurses within the category of healthcare workers, we have formulated the question to what are the differences in vaccine acceptance or hesitancy in nurses compared to other healthcare professionals. Vaccine acceptance was selected as one category, while vaccine indifference, hesitancy or refusal were combined into the other category as the practical outcome is same, ie. non-vaccinated HCW.
METHODS
The eligibility criteria included peer-reviewed original research studies in English language. The aim was to include all geographies.
The lower time limit for the review was set at 2020 as COVID-19 is a disease emerging in late 2019. The search was performed in three healthcare research databases, including PubMed/MEDLINE, PROquest and EBSCO, with most recent search on March 20, 2022.
First, the records were independently screened by two peers based on title and abstract. Fulltext of prescreened articles were assessed prior to inclusion. Duplicities were removed in the process of screening.
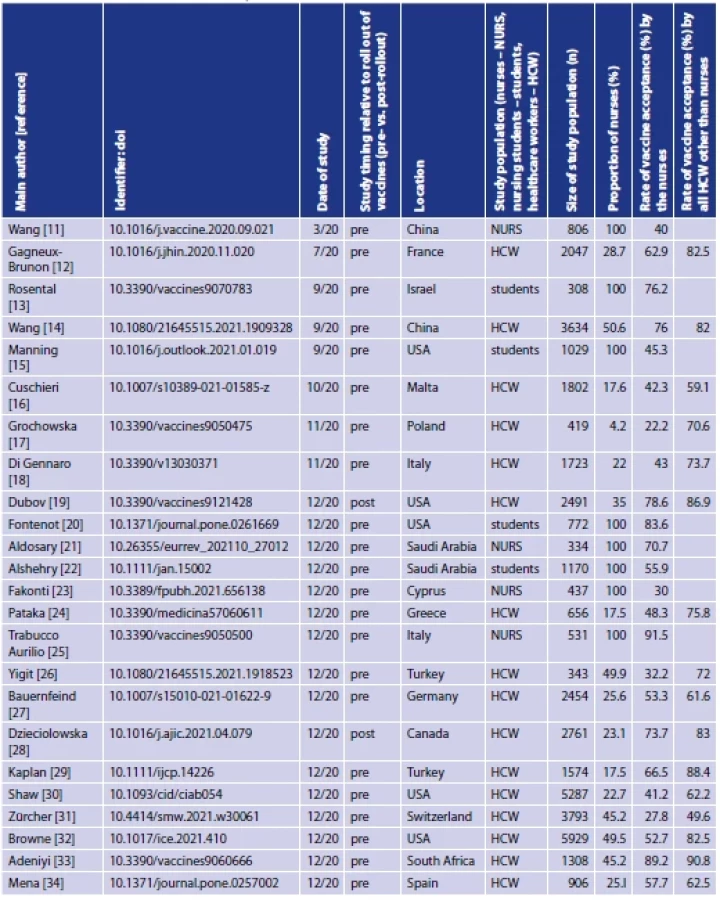
Data extraction was made into a predefined Microsoft Excel spreadsheet (Excel, Microsoft Inc. USA), which included name of the main author, name of the study, doi, publication year, timing of study, date of study relative to local roll-out of vaccines (pre - vs. post-rollout), study design and methodology, geography/location of the study, characteristics of study population, size of study population, proportion of nurses relative to other healthcare professions, rate of vaccine acceptance vs. combined category of waiting, hesitance, and refusal for the nurses and for the other healthcare professions, and categorized main factors and determinants contributing to vaccine acceptance. Handsearch was performed in the references of excluded reviews.
This scoping review focused on identifying any factors that may have influenced the nurses attitudes toward COVID-19 vaccination to form a basis for future studies.
The characteristics of the included studies were summarized by descriptive statistics. Vaccination acceptance rate and vaccination non-acceptance (undetermined, hesitant or refusing) were computed to add to 100 %, if not explicitly stated in the original paper. Rate of vaccination acceptance in HCW other than nurses were calculated from data provided for nurses and all HCW (Excel, Microsoft Inc., USA). Nurses and nursing students were combined in one category since there is a variety of overlapping work and study patterns for nurses in training in different healthcare systems (such as combined type of study and part-time work).
Other variables included geography, type of population, time of study relative to vaccine roll-out. Charts and tables are used to present the results.
The factors associated with COVID-19 vaccination acceptance as opposed to indifference, refusal or hesitancy are reviewed as narrative summary. The identified factors were divided into the three main categories of vaccine hesitancy as specified by the WHO Strategic Advisory Group of Experts on immunization [10], including contextual influences, individual and group influences, and vaccine and vaccination specific issues.
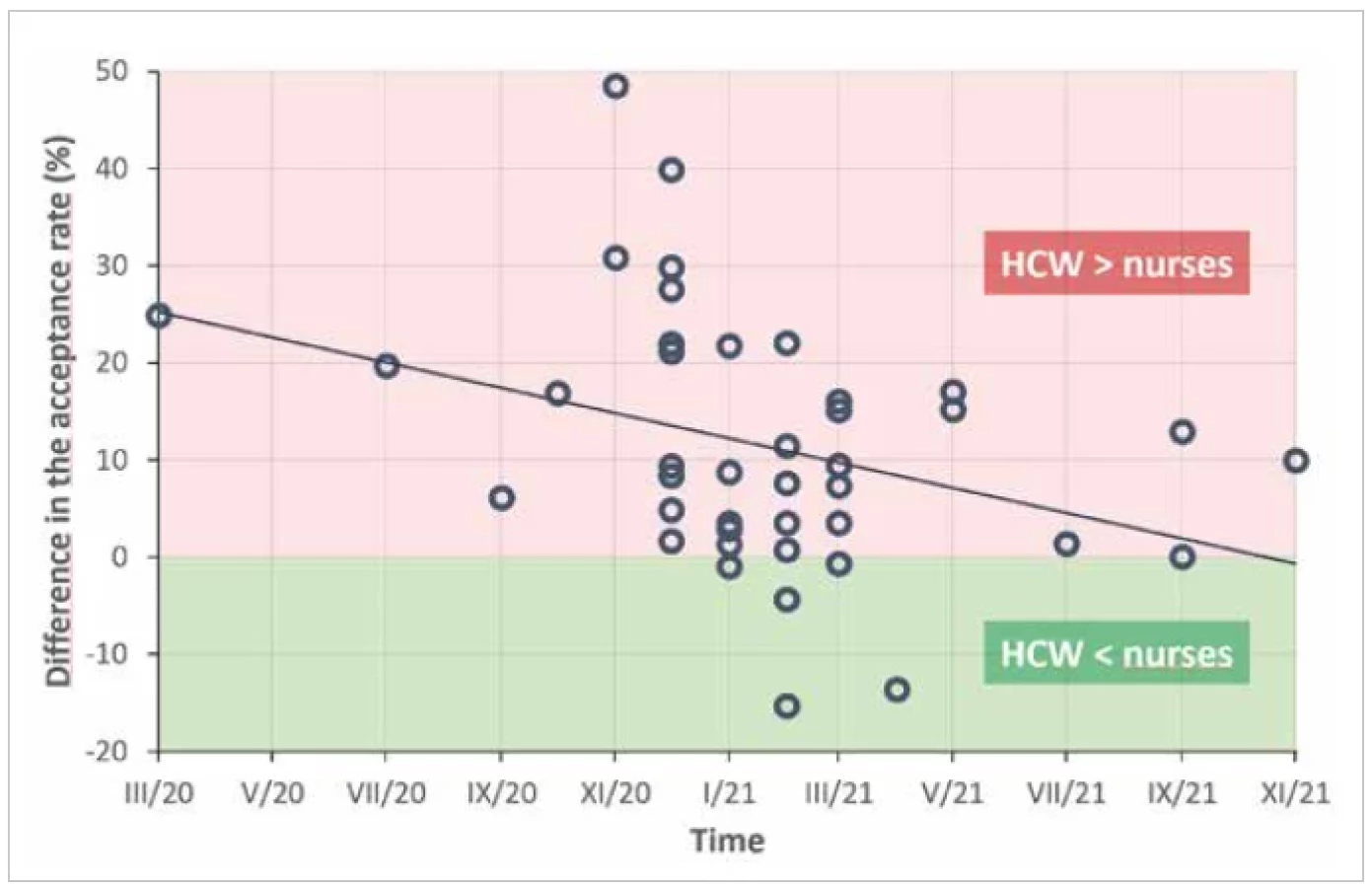
The time evolution of the nurses attitude to vaccine acceptance relative to that of HCW other than nurses was charted post hoc and the significance of the slope parameter of the linear regression model was determined by ANOVA with alpha level 0.05 (SPSS Statistics 24.0, IBM Corp., USA).
Data and graph on real-life Czech HCW COVID-19 vaccination rates were obtained from the Institute of Health Information and Statistics of the Czech Republic (IHIS).
Results
The search in three databases and subsequent selection process provided 58 eligible studies [11–68], all with cross-sectional study design. The process of source search and study selection is depicted in flowchart in Figure 1.

Total 44 studies were organized before the vaccine was available in the given location, 12 after the vaccine roll out, and two studies determined attitude to a booster dose. The time of study, location, numbers of participants (and the proportion of nurses amongst HCW) are shown in Table 1.


The total number of participants included in the review was 95,418 healthcare workers of whom 33,130 were nurses and 7,391 were nursing students. Nine studies took part in the USA, six in China, four in Greece and Saudi Arabia, three in Cyprus, France, Germany, and Italy, two in Albania, Czechia, Ethiopia, Israel, Kosovo, Poland, South Africa and Turkyie, one in Bangladesh, Barbados, Canada, India, Iraq, Kuwait, Malta, Nigeria, Oman, Palestine, Slovakia, South Africa, Switzerland, and United Arab Emirates. One study was organized across 14 Carribean countries.
Factors associated with higher rate of vaccine acceptance in the three WHO domains are listed in Table 2 and summarized below.




Abbreviations: Age+ - vaccination intention increases with age, Age- - vaccination intention decreases with age, M+ - Males have higher vaccination
intention compared to females, F+ - females have higher vaccination intention compared to males, Risk1 – perceived individual risk of severe COVID-19,
fear of getting COVID-19, Risk2 – perceived risk of COVID-19 for other people, living with people at risk of severe disease, Dr+ vs. nurse – doctors higher
intention to vaccination than nurses, HCW+ vs. nurse - all HCW other than nurses had in the study higher intention to vaccination than the subgroup of
nurses, Dr+nurse+ vs. other HCW – doctors and nurses had higher vaccination intention than other healthcare professions, Flu-Vax – having previous
influenza vaccine, Pro-Vax – positive vaccination attitude, general vaccination acceptance and acceptance of previous vaccination programmes, Edu+ -
vaccination acceptance increases with increasing level of education, Edu- - vaccination acceptance decreases with increasing level of education, Work+
- vaccination acceptance increases with longer time in clinical practice, Edu-Vax – high vaccination and/or vaccine knowledge, “vaccine literacy”, „understanding
the vaccine“ or understanding benefits and barriers of vaccination, C+unit – providing direct care for COVID-19 patients, working in a COVID-19
dedicated unit, C-unit – providing care outside of a covid-unit
Context-related factors
Trust in science, in doctors, in experts and in governments were the main contextual factors increasing vaccine acceptance mentioned in the surveys. Access to vaccine and vaccine provision free of charge were significant factors in USA, Bangladesh and China. Trust in official channels of communication as opposed to social media influence was noted. Nurses who declared more trust in pharma industry, vaccine manufacturers or country, where the vaccine was manufactured, were more likely to accept the vaccine. Only few times altruism and collective protection or need to terminate the pandemic was mentioned. Few studies indentified higher acceptance rate in those having in their home someone at risk (n = 5 studies).
Individual and group characteristics
The demographic comparisons have shown that nurses were less likely to accept vaccination compared to doctors and other healthcare professionals especially at the onset of pandemic and before vaccine rollout. This difference decreased with time (Figure 2 and 3) (p = 0.022). The main factors independently associated with higher levels of vaccination acceptance in majority of studies were being male (n = 23 studies), increasing age (n = 25 studies), increasing level of education (n = 7 studies) and increasing number of years in clinical practice (n = 4 studies). Nursing students and nurses attitudes to covid vaccination were similar.

Percieved individual risk of having severe COVID-19 was significant factor in a minority of studies (n = 14).
Differing vaccination intention based on an experience of working in COVID-19 dedicated units was rarely mentioned (chance of vaccine acceptance increased in 5 studies, decreased in one study).
Vaccine and vaccination specific factors
In majority of studies, the main factors associated with higher vaccination intention were trust (or lack of fear) in the vaccine (n = 5 studies), trust in vaccine efficacy and safety (n = 21), or absence of fear of longterm side effects (n = 13). Lack of concerns about the rapid vaccine development was mentioned in some studies (n = 3). Other frequently mentioned factors increasing the intention to vaccinate against COVID-19 were “general positive attitude to vaccination”, “general vaccine acceptance” and “having been vaccinated within previous vaccination programmes” (n = 11 studies), specifically “having had influenza vaccination in previous years” (n = 21 studies). A significant, potentially modifiable cognitive factor, associated with higher vaccine acceptance was “high knowledge of vaccination agenda”, “vaccine literacy”, „understanding the vaccine” or “understanding the benefits and barriers of vaccination” (n = 17 studies).
DISCUSSION
Vaccine hesitancy is one of the top ten threats to global health [69]. The nurses were reported to be more hesitant for COVID-19 vaccine uptake if compared to other healthcare professions. We have found that this was true at the pandemic onset, and during the time period before vaccine roll-out. As time progressed, this difference significantly decreased (see Figure 2 and 3), and this fact was especially apparent in studies done post vaccine roll-out. The data are therefore suggesting that nurses choose a wait-and-see approach toward COVID-19 vaccines (and vaccination in general). The real vaccine uptake by the nurses was higher than their previously declared intention to be vaccinated. In some of the studies nurses initially indicated secondary intention or indifferent attitude, rather than simple vaccine refusal [34, 36, 46]. In one study that was part of an extensive educational programme, all HCW including nurses achieved higher vaccination uptake than what they originally intended [27].
Major contextual factors for vaccination acceptance included trust in official structures and channels of communication as opposed to trusting social media and alternative sources of information. Trust in the country of vaccine manufacture, in the manufacturer and in pharma industry in general was noted in those more willing to be vaccinated. Higher vaccination acceptance was also associated with increasing age, education level and longer work experience, which is all in keeping with this context and we may assume that with more experience and deeper understanding how the healthcare system works (and does not work), one is less prone to look for sources of alternative or conspirational content.
With further pandemic waves and implementation of vaccine mandates by governments or by employers, the real vaccination rate reflected not only the intention or willingness to be vaccinated, but also motivation by being able to work or travel [61]. Higher nurse vaccination intention was noted in regions with higher vaccination intention in general public [63]. On the other side, a certain level of vaccine hesitancy was still persisting even in vaccinated HCWs [66].
When it comes to booster dose acceptance, concerns other than mere questions whether a booster it is needed are the main drivers of reluctance, and may be an important consideration in the planning of messages about booster doses [60].
Previous influenza vaccine uptake as well as participation in other vaccination programmes were indicated as factors increasing vaccine acceptance. This may indicate who may be the “vaccine champions” – people promoting vaccination – in the future: those, who accept vaccine also very likely advocate the vaccine [37]. This is in keeping with the potential of developing nurses’ capacity to be leaders in delivering effective vaccine recommendations to the communities they serve [36].
Another interesting aspect was noted in 17 studies, that identified “vaccine literacy”, “vaccine knowledge” or plain “understanding the vaccine” as an independent factor increasing vaccination acceptance. Indeed, those with low intention to accept the vaccine could be identified as the misinformed, the undecided, the uninformed, or the unconcerned [19]. As the factor of vaccine literacy appears to be modifiable easier than gender, level of education, profession or trust in the government, and faster than age and years in clinical practice, further research into vaccine literacy interventions is warranted. In this review we have identified that it is young and middle aged female nurses including nursing students whose educational needs appear to be unmet and further research should address this, especially realizing how much reliable and culturally informed health communication is vital in influencing positive health behaviour [70].
The findings of occupation-related difference in vaccination acceptance are compatible with real-life data on COVID-19 vaccination in Czech HCWs as reported by IHIS. Figure 4 provided by the courtesy of IHIS shows that the proportions of vaccinated doctors and nurses diverge from the very beginning of vaccination and nurses reach similar vaccine coverage to that of doctors slower both for the basic vaccination and the booster dose. As of 27 September 2022, rates of completed basic COVID-19 vaccination reported by IHIS were in similar range, while booster dose rate was lower in nurses. Currently working Czech doctors completed vaccination in 87.8%, while 75.3% received a booster dose. Currently working Czech nurses completed vaccination in 83.4%, while 61.9% received booster dose. The very first data on 2nd booster bose show similar pattern of early curve divergence.

If nurses tend to wait-and-see at first, but arrive at the end, research then should focus on what needs to be shown so that they feel comfortable accepting the vaccine. As one of the reviewed studies has shown, an ongoing institutional education programme increased vaccine acceptance compared to what nurses claimed in the beginning of such programme [61]. Multicomponent and dialogue-based interventions indeed have been most effective in these settings and this is the way the researchers may turn their attention further on [71].
Limitations
The review included only studies published in English language and some studies published in other languages may have been missed. However, 15,739 out of total 40,521 nurses were surveyed in countries where English is an official language, and 24,782 nurses were in countries where English is not commonly used. Therefore, this linguistic and geographic distribution enables to draw our conslusions to non-English speaking countries as well.
Looking at longitudinal dimension using cross sectional data may have limitations, especially as the studies did not have uniform design and sets of questions, and were performed in various settings. For such variability, however, the findings have shown similar trends and patterns (eg. doctors vs. nurses, age, gender, vaccine literacy) across different countries, healthcare systems and cultures.
Although we have identified multiple factors independently associated with increased COVID-19 vaccine acceptance, we are unable to quantify the size of the effect of individual factors.
There have been other factors that may have influenced the vaccine acceptance, some of them mentioned in the reviewed studies. COVID-19 vaccination intention was influenced by non-medical factors, as COVID-19 has been the first pandemic in the era of widespread use of social media, with related infodemic and desinfodemic features exceeding those of any previous outbreak. Healthcare workers, including nurses, are not spared of this social aspect.
Another limitation of the included studies is the absence of follow-up and real data of vaccine uptake. Therefore, this review can only scope as to what are the declared intentions and which factors are perceived by the nurses and other HCWs to be significant in the process of decision making.
Funding
“Supported by Ministry of Health of the Czech Republic, grant nr. NU21-09-00300. All rights reserved.“
Do redakce došlo dne 6. 9. 2022.
Adresa pro korespondenci:
MUDr. Aleš Chrdle
Nemocnice České Budějovice, a. s.
Boženy Němcové 54
370 01 České Budějovice
e-mail: chrdle@email.cz
Epidemiol Mikrobiol Imunol, 2023;72(1):25–39
Zdroje
1. UNICEF. Facilitator Guide Interpersonal Communication for Immunization: Training for Front Line Workers; UNICEF Europe and Central Asia Region: Geneva, Switzerland, 2019; Available at: https://www.unicef.org/eca/media/8566/file/interpersonal-communication-immunization.pdf.
2. Li T, Qi X, Li Q, et al. A Systematic Review and Meta-Analysis of Seasonal Influenza Vaccination of Health Workers. Vaccines, 2021; 9(10):1104. doi: 10.3390/vaccines9101104.
3. Dini G, Toletone A, Sticchi L, et al. Influenza vaccination in healthcare workers: A comprehensive critical appraisal of the literature. Hum Vaccin Immunother, 2018;14(3):772–789. doi: 10.1080/21645515.2017.1348442.
4. Adli A, Rahimi M, Khodaie R, et al. Role of Genetic Variants and Host Polymorphisms on COVID-19: From Viral Entrance Mechanisms to Immunological Reactions. J Med Virol, 2022. doi: 10.1002/jmv.27615.
5. Mohammed I, Nauman A, Paul P, et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: a systematic review. Hum Vaccin Immunother, 2022 : 1–20. doi: 10.1080/ 21645515.2022.2027160.
6. Boudreau HS, Singh N, Boyd CJ. Understanding the Impact of Social Media Information and Misinformation Producers on Health Information Seeking. Comment on „Health Information Seeking Behaviors on Social Media During the COVID-19 Pandemic Among American Social Networking Site Users: Survey Study“. J Med Internet Res, 2022. doi: 10.2196/31415.
7. Garett R, Young SD. Online misinformation and vaccine hesitancy. Transl Behav Med, 2021;11(12):2194–2199. doi: 10.1093/tbm/ ibab128.
8. ECDC. Vaccine tracker. Available at: https://vaccinetracker.ecdc. europa.eu/public/extensions/COVID-19/vaccine-tracker.html#target-group-tab.
9. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med, 2018;169(7):467–473. doi: 10.7326/M18-0850.
10. World Health Organisation. Report of the SAGEWorking Group on Vaccine Hesitancy. 2014. Available at: https://cdn.who. int/media/docs/default-source/immunization/sage/2014/ october/2-sage-appendicies-background-final.pdf?sfvrsn=2259f1bf_4.
11. Wang K, Wong ELY, Ho KF, et al. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine, 2020;38(45):7049–7056. doi: 10.1016/j.vaccine.2020.09.021.
12. Gagneux-Brunon A, Detoc M, Bruel S, et al. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: a cross-sectional survey. J Hosp Infect, 2021;108 : 168–173. doi: 10.1016/j.jhin.2020.11.020.
13. Rosental H, Shmueli L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines (Basel), 2021;9(7):783. Published 2021 Jul 13. doi: 10.3390/vaccines9070783.
14. Wang J, Feng Y, Hou Z, et al. Willingness to receive SARS-CoV-2 vaccine among healthcare workers in public institutions of Zhejiang Province, China. Hum Vaccin Immunother, 2021;17(9):2926 – 2933. doi: 10.1080/21645515.2021.1909328.
15. Manning ML, Gerolamo AM, Marino MA, et al. COVID-19 vaccination readiness among nurse faculty and student nurses. Nurs Outlook, 2021;69(4):565–573. doi: 10.1016/j.outlook.2021.01.019.
16. Cuschieri S, Grech V. A comparative assessment of attitudes and hesitancy for influenza vis-à-vis COVID-19 vaccination among healthcare students and professionals in Malta. Z Gesundh Wiss, 2021 : 1–8. doi: 10.1007/s10389-021-01585-z.
17. Grochowska M, Ratajczak A, Zdunek G, et al. A Comparison of the Level of Acceptance and Hesitancy towards the Influenza Vaccine and the Forthcoming COVID-19 Vaccine in the Medical Community. Vaccines (Basel), 2021;9(5):475. Published 2021 May 8. doi: 10.3390/vaccines9050475.
18. Di Gennaro F, Murri R, Segala FV, et al. Attitudes towards AntiSARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses, 2021;13(3):371. Published 2021 Feb 26. doi: 10.3390/v13030371.
19. Dubov A, Distelberg BJ, Abdul-Mutakabbir JC, et al. Predictors of COVID-19 Vaccine Acceptance and Hesitancy among Healthcare Workers in Southern California: Not Just „Anti“ vs. „Pro“ Vaccine. Vaccines (Basel), 2021;9(12):1428. Published 2021 Dec 2. doi: 10.3390/vaccines9121428.
20. Fontenot HB, Mattheus DB, Lim E, et al. Undergraduate nursing students‘ COVID-19 vaccine intentions: A national survey. PLoS One, 2021;16(12):e0261669. Published 2021 Dec 22. doi: 10.1371/journal.pone.0261669.
21. Aldosary AH, Alayed GH. Willingness to vaccinate against Novel COVID-19 and contributing factors for the acceptance among nurses in Qassim, Saudi Arabia. Eur Rev Med Pharmacol Sci, 2021;25(20):6386–6396. doi: 10.26355/eurrev_202110_27012
22. Alshehry AS, Cruz JP, Alquwez N, et al. Predictors of nursing students‘ intention to receive COVID-19 vaccination: A multi-university study in Saudi Arabia. J Adv Nurs, 2022;78(2):446–457. doi: 10.1111/jan.15002.
23. Fakonti G, Kyprianidou M, Toumbis G, et al. Attitudes and Acceptance of COVID-19 Vaccination Among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front Public Health, 2021;9 : 656138. Published 2021 Jun 16. doi: 10.3389/ fpubh.2021.656138.
24. Pataka A, Kotoulas S, Stefanidou E, et al. Acceptability of Healthcare Professionals to Get Vaccinated against COVID-19 Two Weeks before Initiation of National Vaccination. Medicina (Kaunas), 2021;57(6):611. Published 2021 Jun 12. doi: 10.3390/ medicina57060611.
25. Trabucco Aurilio M, Mennini FS, Gazzillo S, et al. Intention to Be Vaccinated for COVID-19 among Italian Nurses during the Pandemic. Vaccines (Basel), 2021;9(5):500. Published 2021 May 12. doi: 10.3390/vaccines9050500.
26. Yigit M, Ozkaya-Parlakay A, Senel E. Evaluation of COVID-19 vaccine acceptance of healthcare providers in a tertiary Pediatric hospital. Hum Vaccin Immunother, 2021;17(9):2946–2950. doi: 10.1080/21645515.2021.1918523.
27. Bauernfeind S, Hitzenbichler F, Huppertz G, et al. Brief report: attitudes towards Covid-19 vaccination among hospital employees in a tertiary care university hospital in Germany in December 2020. Infection, 2021;49(6):1307–1311. doi: 10.1007/ s15010-021-01622-9.
28. Dzieciolowska S, Hamel D, Gadio S, et al. Covid-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am J Infect Control, 2021;49(9):1152 – 1157. doi: 10.1016/j.ajic.2021.04.079.
29. Kaplan AK, Sahin MK, Parildar H, et al. The willingness to accept the COVID-19 vaccine and affecting factors among healthcare professionals: A cross-sectional study in Turkey. Int J Clin Pract, 2021;75(7):e14226. doi: 10.1111/ijcp.14226.
30. Shaw J, Stewart T, Anderson KB, et al. Assessment of US Healthcare Personnel Attitudes Towards Coronavirus Disease 2019 (COVID-19) Vaccination in a Large University Healthcare System. Clin Infect Dis, 2021;73(10):1776–1783. doi: 10.1093/ cid/ciab054.
31. Zürcher K, Mugglin C, Egger M, et al. Vaccination willingness for COVID-19 among healthcare workers: a cross-sectional survey in a Swiss canton. Swiss Med Wkly, 2021;151:w30061. Published 2021 Sep 15. doi: 10.4414/smw.2021.w30061.
32. Browne SK, Feemster KA, Shen AK, et al. Coronavirus disease 2019 (COVID-19) vaccine hesitancy among physicians, physician assistants, nurse practitioners, and nurses in two academic hospitals in Philadelphia [published online ahead of print, 2021 Sep 20]. Infect Control Hosp Epidemiol, 2021 : 1–9. doi: 10.1017/ ice.2021.410.
33. Adeniyi OV, Stead D, Singata-Madliki M, et al. Acceptance of COVID-19 Vaccine among the Healthcare Workers in the Eastern Cape, South Africa: A Cross Sectional Study. Vaccines (Basel), 2021;9(6):666. Published 2021 Jun 18. doi: 10.3390/vaccines9060666.
34. Mena G, Blanco B, Casas I, et al. Attitudes of Spanish hospital staff towards COVID-19 vaccination and vaccination rates. PLoS One, 2021;16(9):e0257002. Published 2021 Sep 10. doi: 10.1371/ journal.pone.0257002.
35. Patelarou E, Galanis P, Mechili EA, et al. Factors influencing nursing students‘ intention to accept COVID-19 vaccination: A pooled analysis of seven European countries. Nurse Educ Today, 2021;104 : 105010. doi: 10.1016/j.nedt.2021.105010.
36. Fontenot HB, Mattheus D, Lim E, et al. Assessing licensed nurses COVID-19 vaccine attitudes and intentions: a cross-sectional survey in the state of Hawaii. Hum Vaccin Immunother, 2021;17(11):3933–3940. doi: 10.1080/21645515.2021.1947097.
37. Ahmed G, Almoosa Z, Mohamed D, et al. Healthcare Provider Attitudes toward the Newly Developed COVID-19 Vaccine: Cross-Sectional Study. Nurs Rep, 2021;11(1):187–194. Published 2021 Mar 23. doi: 10.3390/nursrep11010018.
38. Zaitoon H, Sharkansky L, Ganaim L, et al. Evaluation of Israeli healthcare workers knowledge and attitudes toward the COVID-19 vaccine. Public Health Nurs, 2022;39(2):415–422. doi: 10.1111/phn.12987.
39. Zhou Y, Wang Y, Li Z. Intention to get vaccinated against COVID-19 among nursing students: A cross-sectional survey. Nurse Educ Today, 2021;107 : 105152. doi: 10.1016/j.nedt.2021.105152
40. Sun Y, Chen X, Cao M, et al. Will Healthcare Workers Accept a COVID-19 Vaccine When It Becomes Available? A Cross-Sectional Study in China. Front Public Health, 2021;9 : 664905. Published 2021 May 20. doi: 10.3389/fpubh.2021.664905.
41. Rabi R, Maraqa B, Nazzal Z, et al. Factors affecting nurses‘ intention to accept the COVID-19 vaccine: A cross-sectional study. Public Health Nurs, 2021;38(5):781–788. doi: 10.1111/phn.12907.
42. Nohl A, Ben Abdallah H, Weichert V, et al. A Local Survey of COVID-19: Vaccine Potential Acceptance Rate among Personnel in a Level 1 Trauma Center without Severe COVID-19 Cases. Healthcare (Basel), 2021;9(12):1616. Published 2021 Nov 23. doi: 10.3390/healthcare9121616.
43. Xu B, Zhang Y, Chen L, et al. The influence of social network on COVID-19 vaccine hesitancy among healthcare workers: a cross-sectional survey in Chongqing, China. Hum Vaccin Immunother, 2021;17(12):5048–5062. doi: 10.1080/21645515.2021.2004837.
44. Saddik B, Al-Bluwi N, Shukla A, et al. Determinants of healthcare workers perceptions, acceptance and choice of COVID-19 vaccines: a cross-sectional study from the United Arab Emirates. Hum Vaccin Immunother, 2022;18(1):1–9. doi: 10.1080/21645515.2021.1994300.
45. Patelarou A, Saliaj A, Galanis P, et al. Predictors of nurses‘ intention to accept COVID-19 vaccination: A cross-sectional study in five European countries. J Clin Nurs, 2022;31(9-10):1258–1266. doi: 10.1111/jocn.15980.
46. Oliver K, Raut A, Pierre S, et al. Factors associated with COVID-19 vaccine receipt at two integrated healthcare systems in New York City: a cross-sectional study of healthcare workers. BMJ Open, 2022;12(1):e053641. Published 2022 Jan 6. doi: 10.1136/ bmjopen-2021-053641.
47. Khamis F, Badahdah A, Al Mahyijari N, et al. Attitudes Towards COVID-19 Vaccine: A Survey of Health Care Workers in Oman. J Epidemiol Glob Health, 2022;12(1):1–6. doi: 10.1007/s44197-021 - 00018-0.
48. Luma AH, Haveen AH, Faiq BB, Stefania M, Leonardo EG. Hesitancy towards Covid-19 vaccination among the healthcare workers in Iraqi Kurdistan. Public Health Pract (Oxf), 2022;3 : 100222. doi: 10.1016/j.puhip.2021.100222.
49. Kumar R, Beniwal K, Bahurupi Y, et al. Determinants of COVID-19 Vaccination Willingness among Health Care Workers: A Quick Online Survey in India. Korean J Fam Med, 2021;42(6):445–452. doi: 10.4082/kjfm.21.0071.
50. Paris C, Bénézit F, Geslin M, et al. COVID-19 vaccine hesitancy among healthcare workers. Infect Dis Now, 2021;51(5):484–487. doi: 10.1016/j.idnow.2021.04.001.
51. Holzmann-Littig C, Braunisch MC, Kranke P, et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines (Basel), 2021;9(7):777. Published 2021 Jul 12. doi: 10.3390/vaccines9070777.
52. Li XH, Chen L, Pan QN, et al. Vaccination status, acceptance, and knowledge toward a COVID-19 vaccine among healthcare workers: a cross-sectional survey in China. Hum Vaccin Immunother. 2021;17(11):4065-4073. doi:10.1080/21645515.2021.1957415
53. Krishnamurthy K, Sobers N, Kumar A, et al. COVID-19 Vaccine Intent Among Health Care Professionals of Queen Elizabeth Hospital, Barbados. J Multidiscip Healthc, 2021;14 : 3309–3319. Published 2021 Nov 30. doi: 10.2147/JMDH.S336952.
54. Vignier N, Brureau K, Granier S, et al. Attitudes towards the COVID-19 Vaccine and Willingness to Get Vaccinated among Healthcare Workers in French Guiana: The Influence of Geographical Origin. Vaccines (Basel), 2021;9(6):682. Published 2021 Jun 21. doi: 10.3390/vaccines9060682.
55. Wiysonge CS, Alobwede SM, de Marie C Katoto P, et al. COVID-19 vaccine acceptance and hesitancy among healthcare workers in South Africa. Expert Rev Vaccines, 2022;21(4):549–559. doi: 10.1080/14760584.2022.2023355.
56. Amuzie CI, Odini F, Kalu KU, et al. COVID-19 vaccine hesitancy among healthcare workers and its socio-demographic determinants in Abia State, Southeastern Nigeria: a cross-sectional study. Pan Afr Med J, 2021;40 : 10. Published 2021 Sep 3. doi: 10.11604/pamj.2021.40.10.29816
57. Nasir M, Zaman MA, Majumder TK, et al. Perception, Preventive Practice, and Attitude Towards Vaccine Against COVID-19 Among Health Care Professionals in Bangladesh. Infect Drug Resist, 2021;14 : 3531–3540. Published 2021 Aug 31. doi: 10.2147/ IDR.S326531.
58. Al-Sanafi M, Sallam M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines (Basel), 2021;9(7):701. Published 2021 Jun 25. doi: 10.3390/vaccines9070701.
59. Angelo AT, Alemayehu DS, Dachew AM. Health care workers intention to accept COVID-19 vaccine and associated factors in southwestern Ethiopia, 2021. PLoS One, 2021;16(9):e0257109. Published 2021 Sep 3. doi: 10.1371/journal.pone.0257109.
60. Pal S, Shekhar R, Kottewar S, et al. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines (Basel), 2021;9(11):1358. Published 2021 Nov 19. doi: 10.3390/vaccines9111358.
61. Green-McKenzie J, Shofer FS, Momplaisir F, et al. Factors Associated With COVID-19 Vaccine Receipt by Health Care Personnel at a Major Academic Hospital During the First Months of Vaccine Availability [published correction appears in JAMA Netw Open. 2022 Jan 4;5(1):e2147879. JAMA Netw Open. 2021;4(12):e2136582. Published 2021 Dec 1. doi: 10.1001/jamanetworkopen.2021.36582.
62. Gotlib J, Sobierajski T, Jaworski M, et al. „Vaccinate, Do Not Hesitate!“. Vaccination Readiness against COVID-19 among Polish Nursing Undergraduate Students: A National Cross-Sectional Survey. Vaccines (Basel), 2021;9(9):1029. Published 2021 Sep 16. doi: 10.3390/vaccines9091029.
63. Fotiadis K, Dadouli K, Avakian I, et al. Factors Associated with Healthcare Workers‘ (HCWs) Acceptance of COVID-19 Vaccinations and Indications of a Role Model towards Population Vaccinations from a Cross-Sectional Survey in Greece, May 2021. Int J Environ Res Public Health, 2021;18(19):10558. Published 2021 Oct 8. doi: 10.3390/ijerph181910558.
64. Puertas EB, Velandia-Gonzalez M, Vulanovic L, et al. Concerns, attitudes, and intended practices of Caribbean healthcare workers concerning COVID-19 vaccination: A cross-sectional study. Lancet Reg Health Am, 2022;9 : 100193. doi: 10.1016/j. lana.2022.100193.
65. Mohammed R, Nguse TM, Habte BM, et al. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS One, 2021;16(12):e0261125. Published 2021 Dec 17. doi: 10.1371/ journal.pone.0261125.
66. Arif SI, Aldukhail AM, Albaqami MD, et al. Predictors of healthcare workers‘ intention to vaccinate against COVID-19: A cross sectional study from Saudi Arabia. Saudi J Biol Sci, 2022;29(4):2314 – 2322. doi: 10.1016/j.sjbs.2021.11.058.
67. Ulbrichtova R, Svihrova V, Tatarkova M, et al. Acceptance of COVID-19 Vaccination among Healthcare and Non-Healthcare Workers of Hospitals and Outpatient Clinics in the Northern Region of Slovakia. Int J Environ Res Public Health, 2021;18(23):12695. Published 2021 Dec 2. doi: 10.3390/ ijerph182312695.
68. Klugar M, Riad A, Mohanan L, et al. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines (Basel), 2021;9(12):1437. Published 2021 Dec 6. doi: 10.3390/vaccines9121437.
69. World Health Organization Top Ten Threats to Global Health in 2019. 2019 Available at: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
70. Quinn SC, Parmer J, Freimuth VS, et al. Exploring communication, trust in government, and vaccination intention later in the 2009 H1N1 pandemic: results of a national survey. Biosecur Bioterror, 2013;11(2):96–106.
71. Jarrett C, Wilson R, O’Leary M, Eckersberger E, Larson HJ, SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy – A systematic review. Vaccine, 2015;33(34):4180–4190. doi: 10.1016/j.vaccine.2015.04.040.
Štítky
Hygiena a epidemiológia Infekčné lekárstvo MikrobiológiaČlánok vyšiel v časopise
Epidemiologie, mikrobiologie, imunologie

2023 Číslo 1
- Parazitičtí červi v terapii Crohnovy choroby a dalších zánětlivých autoimunitních onemocnění
- Očkování proti virové hemoragické horečce Ebola experimentální vakcínou rVSVDG-ZEBOV-GP
- Koronavirus hýbe světem: Víte jak se chránit a jak postupovat v případě podezření?
Najčítanejšie v tomto čísle
- Črevná mikrobiota, jej vzťah k imunitnému systému a možnosti jej modulácie
- Multilocular infection caused by hypervirulent Klebsiella pneumoniae
- Zvláštnosti Q horečky a dosud zaznamenané humánní případy v České republice
- Charakteristika testu ID-NOW™ určeného k rychlé detekci SARS-CoV-2