
Gastric inflammatory myofibroblastic tumour in a young adult
Inflamatorní myofibroblastický tumor žaludku u mladého dospělého
Úvod: Zánětlivý myofibroblastický nádor (inflammatory myofibroblastic tumour – IMT) žaludku je extrémně vzácný nádor. Autoři prezentují kazuistiku pacienta s primárním IMT žaludku.
Prezentace případu: 24letý muž měl 50mm tumorózní masu na přední stěně střední třetiny žaludku, která byla detekována endoskopií horního gastrointestinálního traktu, s podezřením na gastrointestinální stromální tumor. Byla provedena endoskopická ultrasonograficky řízená aspirace tenkou jehlou a potvrzen zánětlivý myofibroblastický tumor žaludku. Byla provedena laparoskopická klínovitá resekce žaludku.
Diskuze: Primární zánětlivý myofibroblastický tumor žaludku je velmi vzácný mezenchymální novotvar s nejistým maligním potenciálem. Endoskopie horního gastrointestinálního traktu, endoskopická ultrasonografie s následnou aspirací tenkou jehlou se jeví jako metoda volby v předoperační diagnostice submukózních nádorů žaludku. Typ chirurgického výkonu používaného při léčbě primárního IMT žaludku závisí na lokalizaci a velikosti nádoru a také na celkovém stavu pacientů. Míra recidivy po resekci je asi 15–35 %, vzdalené metastázy se objevují u méně než 5 % pacientů. V případě recidivy se obecně doporučuje reexcize, pokud je to možné. Moderní biologická léčba s výrazným efektem zahrnuje léčbu inhibitory ALK (anaplastic lymphoma kinase), případně jinou cílenou léčbu podle molekulárních prediktorů.
Závěr: Když je identifikován submukózní nádor žaludku, je třeba zvážit možnost diagnózy IMT žaludku.
Klíčová slova:
žaludek – tumor žaludku – zánětlivý myofibroblastický tumor – submukózní tumor
Authors:
M. Hošala 1; M. Slezák 1; D. Musová 1; A. Švec 1; M. Mišánik 1; J. Hošalová Matisová 2; J. Miklušica 1; M. Smolár 1
Authors‘ workplace:
Clinic of General, Visceral, and Transplant Surgery, Jessenius Faculty of Medicine, Martin, Comenius University, Bratislava, and University, Hospital Martin, Slovak, Republic
1; Department of Anesthesiology, and Intensive Medicine, Jessenius Faculty of Medicine, Martin, Comenius University, Bratislava, and University, Hospital Martin, Slovak, Republic
2
Published in:
Rozhl. Chir., 2025, roč. 104, č. 9, s. 409-415.
Category:
Case Report
doi:
https://doi.org/10.48095/ccrvch2025409
Overview
Background: The inflammatory myofibroblastic tumour (IMT) of the stomach is an extremely rare tumor. The authors present the case report of a patient with primary gastric IMT.
Case presentation: A 24-year-old man presented with a 50-mm tumorous mass on the anterior wall of the middle third of the stomach, detected by -upper gastrointestinal endoscopy and suspected to be a gastrointestinal stromal tumour. Endoscopic ultrasonography-guided fine needle aspiration was performed and an inflammatory myofibroblastic tumour of the stomach was confirmed. A laparoscopic wedge resection was performed.
Discussion: A primary gastric inflammatory myofibroblastic tumour is a very rare mesenchymal neoplasm of uncertain malignant potential. Upper gastrointestinal endoscopy, endoscopic ultrasonography followed by fine needle aspiration, seems to be a method of choice in the preoperative diagnostic method for submucosal tumors of the stomach. The types of surgical procedures used in the treatment of primary gastric IMTs depend on the localization of the tumor and its size as well as on the general condition of patients. The recurrence rate after resection is about 15–35%, with distant metastases occurring in less than 5% of patients. In the event of a recurrence, re-excision is generally recommended, when possible. Modern biological treatment with significant effects includes the use of ALK inhibitors and other targeted therapy guided by molecular predictors.
Conclusions: When submucosal tumour of the stomach is identified, the possibility of gastric IMT should be considered.
Keywords:
Stomach – inflammatory myofibroblastic tumour – gastric tumour – submucosal tumour
Background
Inflammatory myofibroblastic tumour (IMT) is a very rare mesenchymal neoplasm that has been classified as a neoplastic disease of intermediate biological potential given the low risk of recurrence and metastatic potential. IMT usually occurs in the lungs or the abdominal soft tissues of children and young adults, although a wide anatomic distribution and a broad age range have been documented [1]. Inflammatory myofibroblastic tumor of the stomach is an extremely rare tumor of uncertain etiology with a variety of clinical or imaging features, which makes it difficult to diagnose [2,3]. The authors present the case report of a primary gastric IMT in a 24-year-old patient with Asperger syndrome and schizophrenia.
Case presentation
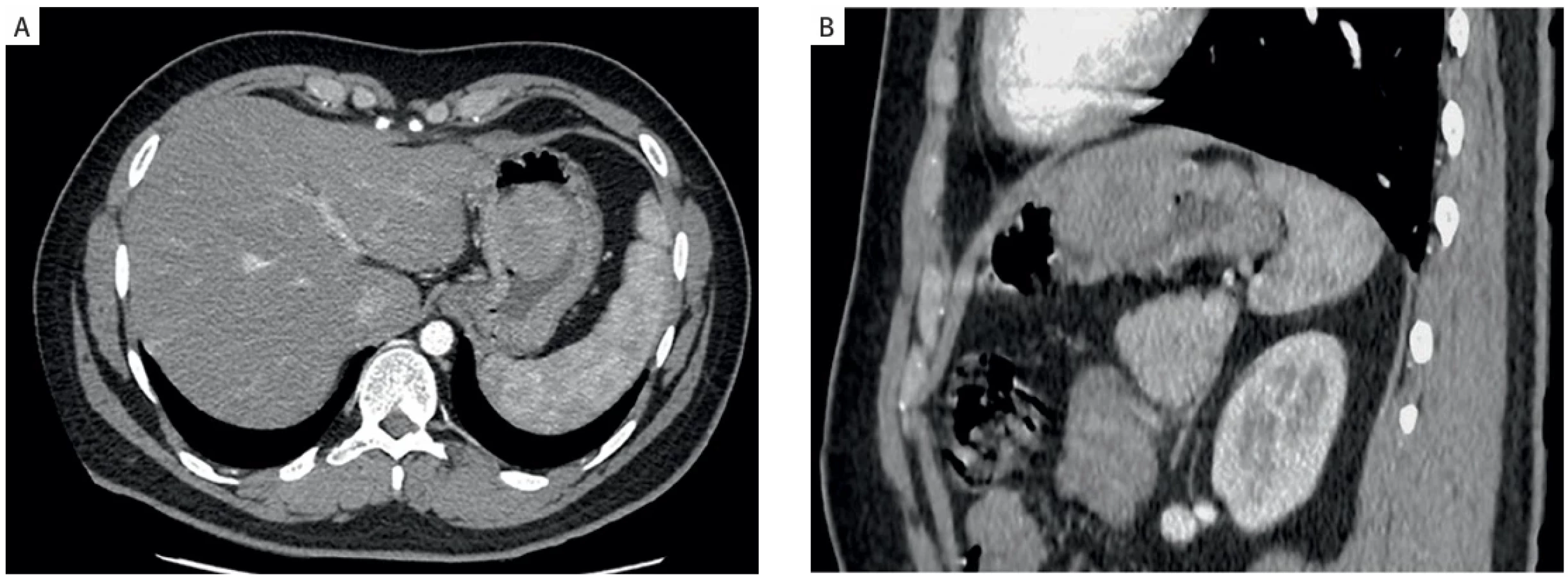
A 24-year-old Caucasian man was examined by a gastroenterologist for anemia and underwent a colonoscopy and upper gastrointestinal endoscopy, revealing a tumorous mass in the upper part of the anterior wall of the stomach. There was no history of abdominal pain, weight loss, or bleeding from gastrointestinal tract (GIT). A contrast-enhanced abdominal CT scan showed a non-homogeneous tumorous mass of 50 × 45 × 47 mm with gastric wall penetration (Fig. 1). Endoscopic ultrasonography-guided fine needle aspiration was performed. Histologically, in the basic hematoxylin-eosin sections, the blood elements and several mildly chronically inflamed, predominantly histiocyte-rich cellular stromal fragments formed by spindle cells, ovoid cells, and a sporadically pleomorphic population, were identified. Immunohistochemically, the expression of SMA and ALK1 (anaplastic lymphoma kinase 1) was identified, with only a rare expression of AE1/AE3 and desmin, and negativity for DOG1, CD34, CD117, CD56, and S100, thus determining the diagnosis of an ALK1+ inflammatory myofibroblastic tumour. Subsequently, laparoscopic surgery was indicated with the tumor localized on the anterior side of the stomach, and a gastric wedge resection was performed. The excision of the tumour from the anterior wall of the stomach was performed using an ultrasonic harmonic device. The opening was closed with a transverse continuous double-layer vicryl suture. The tumor was extracted by minilaparotomy using an endobag extractor. The surgery lasted 135 min, with no complications and minimal blood loss. The macroscopic evaluation showed a semicircular exophytically and polypoidly growing tumor measuring 6.5 × 5 × 3 cm, white in color (Fig. 2). The tumor infiltrated the mucosa through the lamina muscularis propria, ulcerating the gastric mucosa in several places, but the superficial serosa was without invasion and the resection margins were negative. The tumor was composed of interwoven bands of spindle cells with eosinophilic, only focally vacuolated cytoplasm and oval nuclei containing light, finely granular chromatin and small nucleoli. Immunohistochemically, these cells were SMA+, desmin–, ALK+, PDGFR-A+, calponin+, CD34–, S-100–, CD117–, DOG1–. In the peripheral sections of the tumour in particular, numerous inflammatory elements were found (mainly lymphocytes, and less often plasma cells and neutrophils; Fig. 3). Histological and immunohistochemical examinations confirmed the diagnosis of an inflammatory myofibroblastic tumour. The patient recovered well and was uneventfully discharged from our surgical department on postoperative day 6. Currently, 30 months after surgery the patient is without any clinical signs of complications and there is no evidence of pathological findings on the follow-up CT scan and upper gastrointestinal endoscopy.


Discussion
IMT was first reported in two cases of benign pulmonary spindle cell tumours by Brunn in 1939 [4]. The primary gastric inflammatory myofibroblastic tumour is a very rare mesenchymal neoplasm of uncertain malignant potential characterized morphologically by proliferating spindle cells with myofibroblastic differentiation admixed with a prominent inflammatory component giving rise to secondary constitutional symptoms [5]. In 2021, Hajong published that IMT may be predisposed by infectious, autoimmune, or neoplastic conditions [6].
Its etiology and pathogenesis are still controversial. In 2008, Gleason described a chromosomal variation of the ALK gene as one of its potential etiological agents. Rearrangements involving the ALK locus on chromosome 2p23 have been documented in both pulmonary and extrapulmonary IMTs, providing further support for the neoplastic nature of these lesions and their distinction from other “inflammatory pseudotumors” [7]. Infections such as mycobacteria, Epstein-Barr virus, actinomycetes, Nocardia, and Helicobacter pylori are also suggested as etiological agents [8]. Making an accurate preoperative diagnosis of IMT is difficult. Patients with IMT sometimes present with anemia in their laboratory analysis; some of the patients are asymptomatic. In academic literature, a large variety of symptoms have been described. The most common symptoms include: abdominal pain, anemia, body weight loss, GIT bleeding, malaise, and abdominal discomfort [9]. Jadhav in 2017 and Hattori in 2024 reported in their reviews that almost 50% of patients suffered abdominal pain as the main symptom [2,9]. In contrast, even though our patient had a large tumor in his stomach, he had no abdominal pain. Anemia, as the main symptom was referred to in about 30% of all cases described by Hattori. Hence, according to several authors, upper gastrointestinal endoscopy and endoscopic ultrasonography appear to be the gold standard as an initial diagnostic step. Fine needle aspiration seems to be a method of choice in the preoperative diagnostic method of submucosal tumours of the stomach. To date, more than 40 cases of inflammatory myofibroblastic tumour of the stomach have been described in academic literature. A complete surgical resection of the tumour is required since residual tumors can cause local recurrence [2]. The extent of optimal surgical resection remains unclear [10]. More than 50% of patients undergoing surgical treatment for IMT have undergone partial gastrectomy. In his case report of a 69-year-old man, Hattori reported a partial gastric resection. In contrast, Bjelovic in his case report performed a subtotal gastrectomy with D2 lymph node dissection and Roux-en-Y reconstruction. Only two cases are described in literature as being treated with endoscopic mucosal resection [11]. The types of surgical procedures used in other cases of primary gastric IMTs depended on the tumour’s localization and size, as well as the general condition of the patients. The recurrence rate after resection is about 15–35%, with most cases showing local recurrence [11–13]. The distant metastases are rare (less than 5%) and most commonly involve the lungs, brain, liver, and bone [15]. Although several reports suggested that the anatomic site of IMT is associated with the recurrence rate, there are no detailed reports of the postoperative recurrence of primary gastric IMT [11]. The National Comprehensive Cancer Network (NCCN) guidelines recommend ALK inhibitors as first-line systemic therapy for advanced-stage, recurrent, metastatic, or inoperable IMTs with ALK fusions [15]. Tyrosine kinase inhibitors have also demonstrated significant efficacy in ALK-positive IMTs. However, treatment options for ALK-negative or refractory cases remain limited, highlighting the need for alternative targeted therapies [15]. IMT of the stomach has a relatively good prognosis and should be considered in the differential diagnosis of soft tissue tumours in the stomach to avoid unnecessary aggressive therapy. Due to the limited number of cases, larger organ-specific prospective case series with long-term follow-up are necessary [5].
Conclusion
Inflammatory myofibroblastic tumors are a rare group of neoplasms, which have not been investigated in detail due to the difficulty of collecting a large number of cases [17]. Primary gastric IMT is a very rare disease and very closely mimics gastric gastrointestinal stromal tumour. A post‑operative immunohistochemistry examination can differentiate IMT from gastrointestinal stromal tumour. Complete surgical resection, with negative surgical margins, is considered a primary and efficient treatment for IMTs. For advanced stages, ALK inhibitors, have demonstrated efficacy in treating ALK-positive IMTs. The integration of molecular insights with advanced diagnostic and therapeutic strategies will be essential for improving patient outcomes and advancing precision medicine [16]. Gastric IMT should be one of the differential diagnoses in cases of tumours with exophytic growth arising from the stomach [6].
Consent
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Conflict of interests
The authors declare that they have no conflict of interest related to the creation of this article, and that this article has not been published in any other journal with access to congress abstracts.
Sources
1. Gros L, Dei Tos AP, Jones RL et al. Inflammatory Myofibroblastic Tumour: State of the Art. Cancers 2022; 14(15): 3662. doi: 10.3390/cancers14153662.
2. Hattori T, Tanizawa Y, Shimoda T et al. Gastric inflammatory myofibroblastic tumor: a case report. Surg case rep 2024; 10(1): 62. doi: 10.1186/s40792-024-01844-7.
3. Katakwar A, Gedam BS, Mukewar S et al. Primary gastric inflammatory myofibroblastic tumor in an adult – case report with a brief review. Indian J Surg Oncol 2014; 5(1): 66–70. doi: 10.1007/s13193-014-0296-5.
4. Brunn H. Two interesting benign lung tumors of contradictory histopathology: Remarks on the necessity for maintaining the chest tumor registry. J Thorac Surg 1939; 9(2): 119–131. doi: 10.1016/S0096-5588(20)32030-4.
5. Panigrahi C, Shahin M, Nayak HK et al. Gastric inflammatory myofibroblastic tumor in a young child – a case report and literature review. Indian J Pathol Microbiol 2023; 66(2): 428–430. doi: 10.4103/IJPM.IJPM_691_21.
6. Hajong R, Newme K, Khongwar D. Primary inflammatory myofibroblastic tumor of the stomach – report of a very rare case. J Family Med Prim Care 2021; 10(1): 552–553. doi: 10.4103/jfmpc.jfmpc_1126_20.
7. Gleason BC, Hornick JL. Inflammatory myofibroblastic tumors: where are we now? J Clin Pathol 2008; 61(4): 428–437. doi: 10.1136/jcp.2007.049387.
8. Jadhav M, Harvi R, Patil R et al. Inflammatory myofibroblastic tumor of the stomach presenting as an exophytic mass – a diagnostic dilemma. Turk Patoloji Derg 2019; 35(2): 151–156. doi: 10.5146/tjpath.2017.01388.
9. Bjelovic M, Micev M, Spica B et al. Primary inflammatory myofibroblastic tumor of the stomach in an adult woman: a case report and review of the literature. World J Surg Oncol 2013; 11(35): 1–6. doi: 10.1186/1477-7819-11-35.
10. Uno H, Takahara Y, Nishida T et al. A case of laparoscopic local resection of the stomach for an inflammatory myofibroblastic tumor. Gan To Kagaku Ryoho 2019; 46(13): 2054–2056.
11. Cofin CM, Fletcher JA. Infammatory myofibroblastic tumour. In: Fletcher CD, Unni KK, Mertens F (eds). World Health Organization classification of tumours: tumors of soft tissue and bone. Lyon: IARC Press 2002. 91–93.
12. Shi H, Wei L, Sun L et al. Primary gastric inflammatory myofibroblastic tumor: a clinicopathologic and immunohistochemical study of 5 cases. Pathol Res Pract 2010; 206(5): 287–291. doi: 10.1016/j.prp.2009.09.002.
13. Hayashi M, Kawakubo H, Mayanagi S et al. Gastric inflammatory myofibroblastic tumor treated with combined laparoscopic and endoscopic gastric wedge resection: a case report. World J Surg Oncol 2018; 16(1): 161. doi: 10.1186/s12957-018-1460-0.
14. Cheng B, Yang C, Liu Z et al. Primary gastric inflammatory myofibroblastic tumor: a case report. Medicine (Baltimore) 2018; 97(50): e13423. doi: 10.1097/MD.0000000000013423.
15. National Comprehensive Cancer Network®. NCCN Clinical practice guidelines in oncology: Uterine Neoplasms (version 2.2024). Philadelphia (USA): NCCN 2024 [online]. Available from: https://www.nccn.org/login?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/uterine.pdf.
16. Choi JH. Inflammatory myofibroblastic tumor: an updated review. Cancers 2025; 17(8): 1327. doi: 10.3390/cancers17081327.
17. Siemion K, Reszec-Gielazyn J, Kisluk J et al. What do we know about inflammatory myofibroblastic tumors? – A systematic review. Adv Med Sci 2022; 67(1): 129–138. doi: 10.1016/j.advms.2022.02.002.
Miroslav Slezák, MD, PhD
Clinic of General, Visceral and Transplant Surgery
Jessenius Faculty of Medicine, Martin
Comenius University, Bratislava
Kollárova 2
036 59 Martin
Slovak Republic
slezak27@uniba.sk
ORCID of authors
M. Hošala 0000-0002-7981-7501
M. Slezák 0009-0004-8111-3767
J. Hošalová Matisová 0009-0000-6436-6843
J. Miklušica 0009-0003-6442-4064
M. Smolár 0000-0002-7381-5513
Labels
Surgery Orthopaedics Trauma surgeryArticle was published in
Perspectives in Surgery

2025 Issue 9
- Safety and Tolerance of Metamizole in Postoperative Analgesia in Children
- Metamizole in perioperative treatment in children under 14 years – results of a questionnaire survey from practice
- Obstacle Called Vasospasm: Which Solution Is Most Effective in Microsurgery and How to Pharmacologically Assist It?
- Possibilities of Using Metamizole in the Treatment of Acute Primary Headaches
- Current Insights into the Antispasmodic and Analgesic Effects of Metamizole on the Gastrointestinal Tract
Most read in this issue
- Emergencies in proctology
- Periappendiceal infiltrate – conservative therapy – retrospective data analysis and overview of literature
- Robotic colonic resection – our experiences after 3 years to the elbow
- Total pancreatectomy with Langerhans islets autotransplantation for pancreatico-pleural fistula 2 years after pancreatoduodenectomy for chronic pancreatitis