
First experience with dorsal cochlear nuclei monitoring in vestibular schwannoma surgery in the Czech Republic
Authors:
M. Voldřich 1; A. Vlasák 2; J. Betka 1; B. Kindlová 1; J. Dittrichová 1; L. Galiyeva 1; Z. Fík 1
Authors‘ workplace:
Department of Otorhinolaryngology, Head and Neck Surgery, First Medical Faculty, Charles University, University Hospital Motol and Homolka, Prague, Czech Republic
1; Department of Neurosurgery, Second Medical Faculty, Charles University, University Hospital Motol and Homolka, Prague, Czech Republic
2
Published in:
Cesk Slov Neurol N 2026; 89(3): 170-177
Category:
Original Paper
doi:
https://doi.org/10.48095/cccsnn2026170
Overview
Aim: Hearing preservation has become a major objective in vestibular schwannoma surgery, as postoperative hearing outcomes significantly affect patients’ quality of life. Standard intraoperative monitoring techniques – brainstem auditory evoked potentials (BAEP) and less commonly used cochlear nerve action potentials (CNAP) – have important limitations, particularly in speed, stability, and susceptibility to noise. Dorsal cochlear nucleus action potential (DNAP) monitoring is a newer technique that enables near-continuous assessment of cochlear nerve function. The aim of this work is to present the first experience with DNAP monitoring in the Czech Republic and evaluate its feasibility, signal stability, and usefulness during vestibular schwannoma resection. Methods: DNAP monitoring was attempted in five patients undergoing retrosigmoid transmeatal resection of vestibular schwannoma between October 2024 and September 2025. Three types of electrodes (Nihon Kohden, Inomed, Spes Medica) were used. BAEP and CNAP were recorded simultaneously. CNAP and DNAP required averaging of only 40 responses, whereas BAEP required 600. Results: Electrode placement could not be safely achieved in two cases. In the three successfully monitored patients, DNAP and CNAP provided stable signals throughout the procedure, even in situations where BAEP could not produce a reliable response. Changes in DNAP amplitude and latency correlated with cochlear nerve condition at the end of surgery. There were notable differences in electrode handling and stability: the Nihon Kohden electrode was easiest to position and most stable. Conclusion: DNAP is a feasible and promising intraoperative monitoring modality, particularly when BAEP responses are unstable or unreliable. In our first three cases, DNAP delivered valuable and continuous information about cochlear nerve function. Further prospective studies are needed to define its limitations, optimal use, and clinical value.
Keywords:
vestibular schwannoma – hearing preservation – cochlear nuclei monitoring – BAEP
Introduction
Hearing preservation has become a critical objective in vestibular schwannoma surgery, as postoperative hearing function is a major determinant of patients’ quality of life, communication ability, and psychosocial well-being.
Two of the most common techniques for auditory monitoring in vestibular schwannoma resection surgery are brainstem auditory evoked potential (BAEP) and cochlear nerve action potential (CNAP). BAEPs are a non-invasive combination of near - and far-field recordings monitoring the auditory pathway from the proximal cochlear nerve to the brainstem. Since BAEPs are recording far-field potentials, they require a large number of averaged trials (500–1,500; 35–135 s). This means they can’t provide real-time feedback that is essential in detecting damage to the cochlear nerve. Another disadvantage lies in the low signal-to-noise ratio. This is especially relevant in intraoperative monitoring due to the increased amount of noise generated by different surgical instruments leading to inconclusive and unstable BAEP responses. This becomes even more apparent in patients with vestibular schwannoma, where the BAEP recording may already be altered from the beginning by the primary pathology [1].
Cochlear nerve action potential records near-field responses directly from the cochlear nerve and hence does not require extensive averaging (3–4 s) of trials thereby providing near real-time monitoring [2]. Due to the proximity of the electrode, the response amplitude is significantly higher than BAEP waves. The main disadvantages of CNAP include the need to localize the cochlear nerve prior to measurement, which is apparent in large tumors. There are two options. One includes continuous monitoring with the electrode placed on/near the cochlear nerve. In this case, the electrode is frequently displaced during surgery and can lead to false-positive changes of response [3]. The second possibility is intermittent measurement with a ball electrode, which is normally placed on the nerve during surgery, with the disadvantage of losing continual information about the hearing status [4].
Dorsal cochlear nucleus action potential (DNAP) monitoring allows near real-time monitoring of cochlear nerve function [5] by recording near-field potentials from the dorsal cochlear nucleus. It overlaps the problem of the CNAP technique – stability of the electrode and like CNAP, it requires significantly fewer trials compared to BAEP. In our experience, 40 trials are sufficient to capture and provide a response every 3–4 s. The ability to detect changes in the DNAP signal in real-time is crucial for preventing further damage to the cochlear nerve by allowing surgeons to let the nerve recover [6]. One advantage of DNAP is the ability to map the cochlear nerve using electrical stimulation along the entire relevant trajectory [5]. A similar function can be achieved with the combination of bimodal action potential monitoring, where DNAP provides real--time monitoring of cochlear nerve function and CNAP monitoring is used for localization (useful especially in large tumors).
Materials and methods
At the Department of Otorhinolaryngology and Head and Neck Surgery, First Faculty of Medicine, Charles University and Motol University Hospital, Prague, DNAP monitoring in the lateral recess of the fourth ventricle was attempted in five patients, after informed consent signature, between October 2024 and September 2025.
All five procedures were performed via a retrosigmoid transmeatal osteoplastic craniotomy. The surgical technique used at this institution has been described previously [7]. After opening of the dura and releasing of the CSF from the arachnoid cistern, the lateral recess is approached following the direction of the IXth cranial nerve (described elsewhere) [8]. All attempts have been performed by a skilled neurosurgeon (A.V.), experienced in the surgery of auditory brainstem implants from the last 3 years at the authors’ center. Moreover, the authors’ institution has the unique historical experience with auditory brainstem implants in adults within the Czech Republic [9].
Neuromonitoring was performed using Inomed ISIS Xpert neuromonitoring (Inomed Medizintechnik GmbH, Emmendingen, Germany). Auditory monitoring modalities included BAEP, CNAP and DNAP for auditory evoked potentials monitoring (AEP). Furthermore, facial nerve monitoring including facial motor evoked potentials have been used.
For BAEP, the active electrodes were placed on the contralateral mastoid and directly behind the ipsilateral ear to avoid collision with the surgical field. CNAP was recorded with a recording electrode manually from the cochlear nerve. A special electrode for DNAP was placed in the lateral recess of the fourth ventricle. A reference electrode was placed on the vertex (Cz) and a grounding electrode was placed on the forehead (Fz), which were shared for all auditory evoked potentials.
Acoustic click stimulation to the ipsilateral ear had an intensity of 95 dB HL and a frequency of 14.3 Hz for BAEP, and 11.1 Hz CNAP and DNAP, resp. The contralateral ear was masked with gaussian noise at 60 dB. The BAEP response was averaged for 600 trials while CNAP and DNAP were averaged for 40 trials. Low-pass filter was set to 3,000 Hz and a high-pass filter was set to 150 Hz for all AEP.
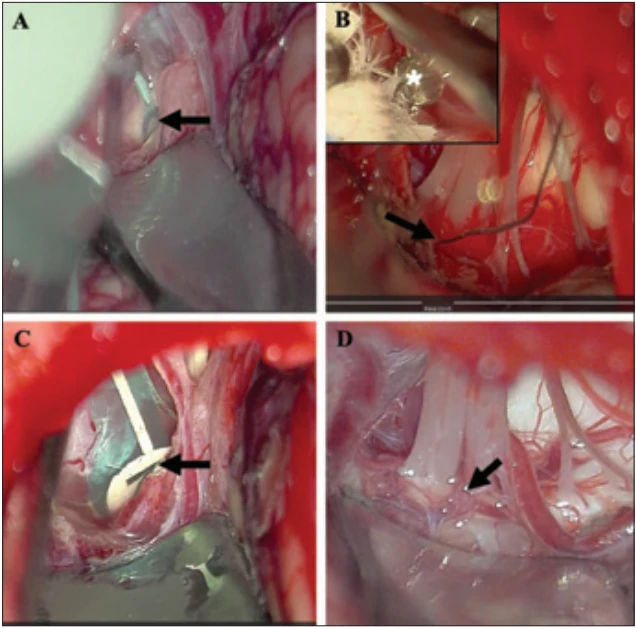
Three types of electrodes were used:
1) Platinum STRIP electrode (Spes Medica S.r.A., Genova, Italy); (Fig. 1C)
2) Ball electrode (Inomed Medizintechnik GmbH, Emmendingen, Germany) (Fig. 1B);
3) DNAP electrode (Nihon Kohden Corporation, Tokyo, Japan) (Fig. 1A).
Results
DNAP monitoring was attempted in five patients. In two cases, correct electrode placement could not be achieved safely; in one of them, this was due to overlapping vessels obstructing the recess opening (Fig. 1D), and in the second case, it was due to challenging electrode handling (Inomed). A summary of the three successful case reports is presented below.
Case 1 – male, 47 years
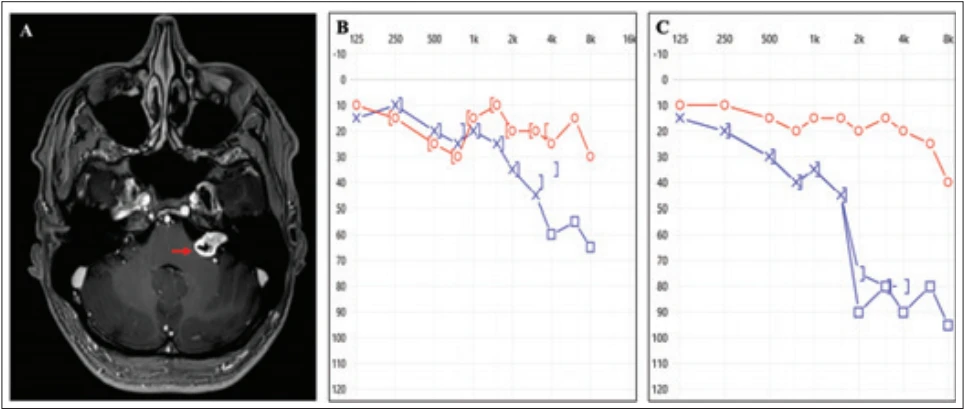
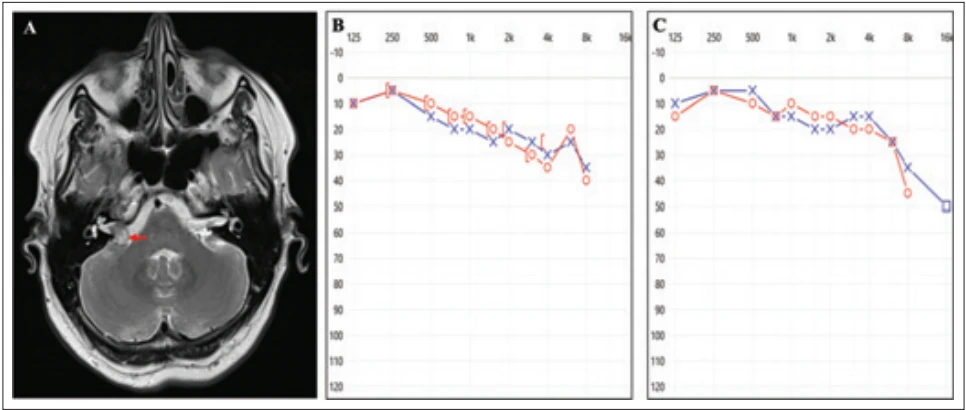
A patient with a left-sided vestibular schwannoma, Koos grade III, measuring 19 × 12 × 12 mm (Fig. 2A), was referred for progressive hearing deterioration (Fig. 2B). Considering the tumor size, two management options were discussed – observation or microsurgical resection with an attempt to preserve hearing. The patient opted for surgery.
An uncomplicated retrosigmoid approach with intraoperative DNAP monitoring (Nihon Kohden electrode [Fig. 1A]) was performed. Gross total tumor removal was achieved with hearing preservation (Fig. 2C). The postoperative pure tone average (PTA) increased from 36 dB to 55 dB. Speech audiometry was not performed because the patient is not a native Czech speaker.
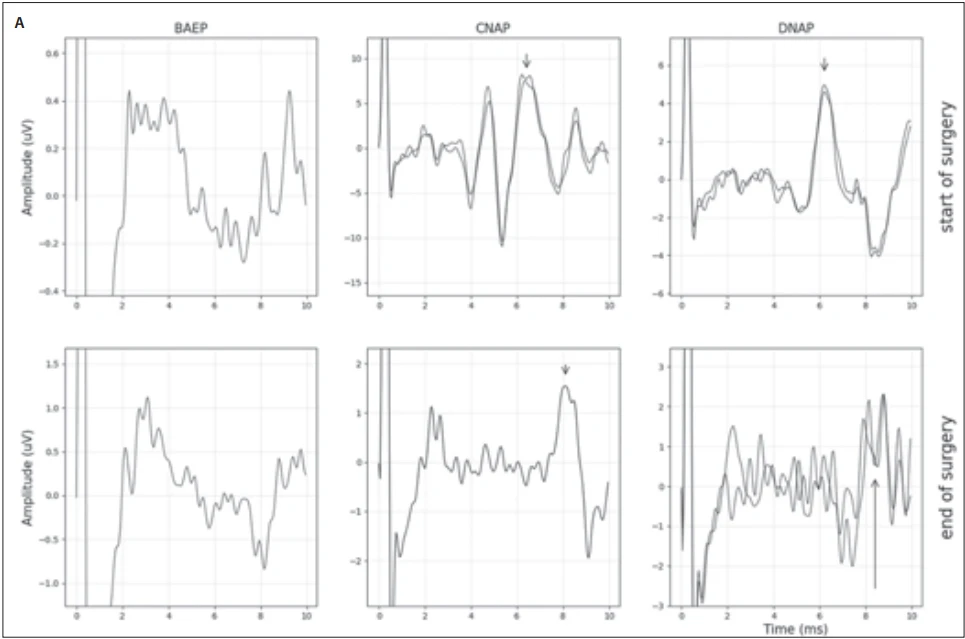
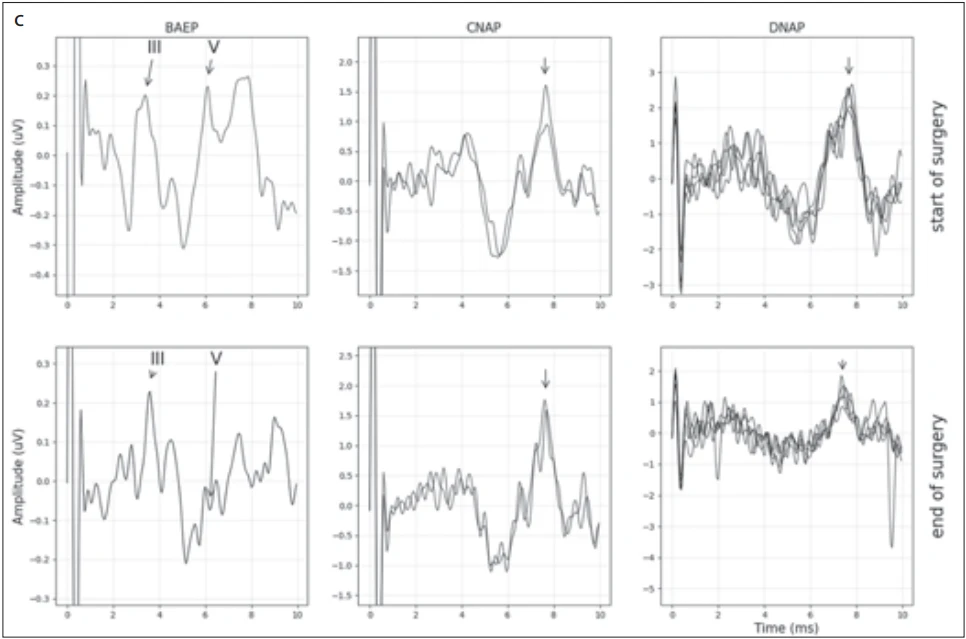
Preservation of the cochlear nerve was challenging. Intraoperative monitoring showed a progressive decline in both CNAP and DNAP amplitude and an increase in response latency throughout surgery. Despite this trend, reproducible DNAP responses (corroborated by CNAP) were obtained at the end of the surgery. The significantly reduced amplitude of these final responses, however, indicated impaired function of the cochlear nerve.
BAEP responses were unstable for the entire duration of the surgery apart from wave I (Fig. 3A).
Case 2 – female, 53 years
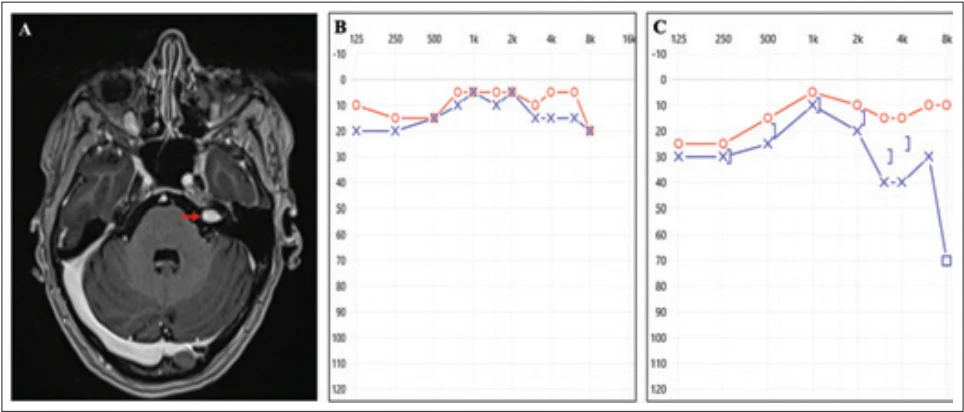
A patient with a growing right-sided vestibular schwannoma (Koos grade II, 13 × 8 × 8 mm; Fig. 4A) was counselled regarding three management options: continued observation, hearing preservation surgery, or stereoradiotherapy.
Microsurgical resection was performed without complications using intraoperative DNAP monitoring with an Inomed ball electrode (Fig. 1B). Gross total tumor removal was achieved. Electrode insertion was technically demanding due to handling difficulties and an inadequately rigid leading wire. Hearing was preserved, with pure tone average improving from 23 dB preoperatively to 15 dB postoperatively; word recognition (WRC) at 60 dB remained 100% (Fig. 4B, C).
Both DNAP and CNAP responses remained reproducible during the entire surgery, indicating preserved cochlear nerve function. While some variation in DNAP amplitude and latency was observed intraoperatively, the final responses recorded before closure were comparable to those obtained at baseline.
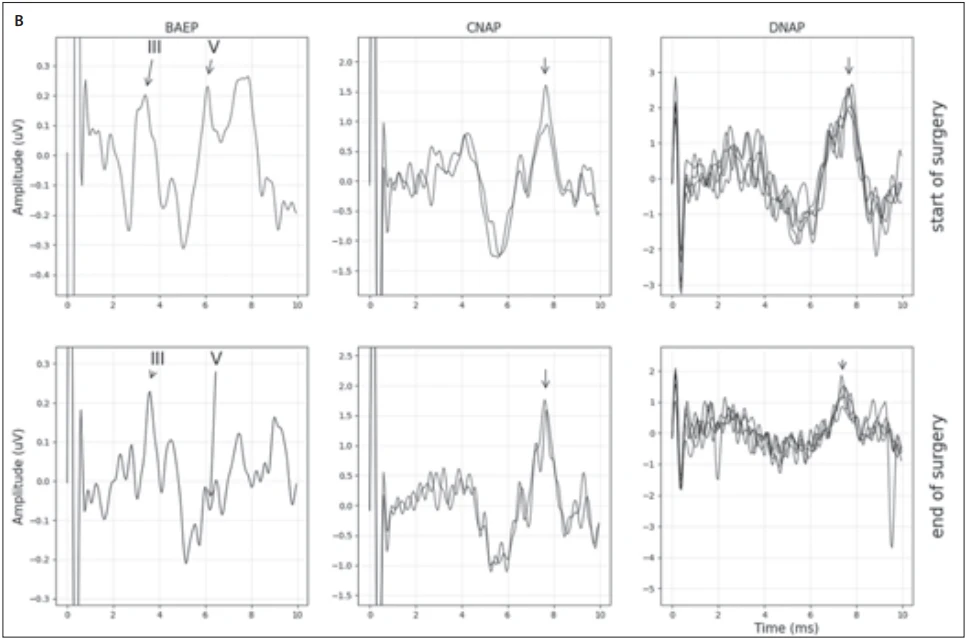
A stable BAEP baseline response was established at the start of surgery and a comparable response with increased amplitude of wave III was recorded at the end of the surgery. During the procedure, however, the signal was contaminated with noise and failed to produce a stable response (Fig. 3B).
Case 3 – female, 46 years
A patient with a small left-sided vestibular schwannoma that had progressed from Koos grade I to Koos grade II (10 × 6 × 5 mm; Fig. 5A) and suitable hearing (PTA 11 dB, WRC 100%; Fig 5B) was counselled regarding three management options, including a wait-and-rescan strategy. The patient elected to undergo microsurgery with the aim of hearing preservation.
In this case, a platinum strip electrode (Fig. 1C) was used, providing excellent flexibility. The only disadvantage observed was the elastic sheath along the wire, which tended to slip out of the wound. Suitable hearing was preserved postoperatively (PTA 27 dB; WRC 100%; Fig. 5C)
Reproducible DNAP and CNAP responses were maintained throughout the operation, indicating preserved cochlear nerve function. An initial drop in DNAP amplitude was observed in the first five minutes following electrode implantation, presumably from movement of the electrode. The responses subsequently stabilized and remained constant for the remainder of the surgery. BAEP recordings were contaminated with noise and no reproducible responses were obtained (Fig. 3C).
Discussion
Modern microsurgical techniques and intraoperative monitoring of auditory brainstem responses and cochlear nerve action potentials have improved the likelihood of maintaining serviceable hearing, particularly in small to medium-sized tumors (e. g., prognostic factors such as tumor size and preoperative hearing status strongly impact outcome) [10,11]. However, hearing integrity does not depend solely on immediate postoperative results. As shown by Fík et al., even when hearing is initially preserved, delayed deterioration over months to years is a significant concern [10]. For example, a systematic review reported that for microsurgery, the estimated rate of maintaining serviceable hearing falls to ~32 % at 10 years post--surgery [12]. This highlights that hearing preservation is not only a surgical challenge, but also a long-term functional objective requiring careful patient selection, meticulous microsurgical technique, and structured postoperative audiological follow-up. Consequently, the balance between radical tumor removal and preservation of hearing function remains a central and evolving dilemma in contemporary vestibular schwannoma management.
Although cochlear nuclei monitoring is rarely used, it has been described by Møller and Jannetta in 1983 [13], and it was subsequently further developed by the Hannover school [14]. The revival of this technique began with the work of Nakatomi et al., who reported significant improvement in hearing preservation compared to the group without cochlear nuclei monitoring (73.7 vs. 27.8%) with further improvement to 79% in the subsequent study [15,16]. Similar promising results have been reported by a collaborating center (Copenhagen). In the Denmark series, the introduction of cochlear nucleus monitoring increased serviceable-hearing preservation from 53% to 77%, underscoring its substantial impact on functional outcomes [17].
This is the first report of this technique used in the Czech Republic. It has been successfully used in three patients with three different types of electrodes. The purpose of using a different electrode was to try to solve the problems, which we encountered during the whole process. The first electrode from Nihon Kohden is designed specifically for this technique, so it outperforms the other two in case of handling and stability in the operation field. The main drawback is the price for a single-use product, which is more than 10 fold higher compared to the other two options. The ball electrode from Inomed had very good stability when placed in the foramen of Luschka, but the handling was very difficult in both cases and in one of them, it compromised the attempt to insert the electrode into the proper place. Moreover, the metallic wire needed special attention during its course along the cerebellum. The last Platinum STRIP electrode required thinning of the silastic covering, but it fits the lateral recess very well and its placing was smooth. The disadvantage can be found in the highly elastic wire, witch has a tendency to dislocate the electrode from the targeted place. Those issues are probably responsible for the low utilization of this technique among professionals worldwide. Locally specific difficulties lie also in the small national market, which makes it sometimes tricky to find access to all the equipment, especially when its usage is predicted to be low.
In one case, we found the preparation of the entry zone to the lateral recess risky due to the overlapping vessels, which crossed the lower cranial nerve bundle. In case of bleeding, the neural structures would be at excessive risk and it was not advisable to continue with other attempts. However, precise anatomical description of the foramen Luschka approach exists in the literature [18], although difficulties with proper insertion are described frequently in the auditory brainstem implant papers, suggesting even failure of the implantation itself [19,20].
Conclusion
Hearing preservation is still a challenge in the everyday vestibular schwannoma routine. One of the key aspects remains in electrophysiological perioperative assessment, but its predictive validity is still debatable. The important shift comes with detection of stimuli directly from the cochlear nerve and even from dorsal cochlear nuclei. As it is not a commonly used technique, the result seems to be promising, forcing us to work on deeper utilization. The main drawback lies in poor accessibility of a standardized electrode and the necessity for expertise in advanced posterior skull base surgery.
Acknowledgement
The authors would like to thank Professor Cordula Matthies (Würzburg, Germany) and Professor Per Caye-Thomasen (Copenhagen, Denmark) for their invaluable technical support and assistance with the implementation of this new method.
Ethical principles
The entire study was conducted in accordance with the Helsinki Declaration of 1975 (as revised in 2004 and 2008), and was approved by the Ethics Committee of the University Hospital Motol and Homolka and 2nd Faculty of Medicine Charles University in Prague (EK-20/26, 29. 1. 2026).
Financial support
This work was supported by the Cooperation Program, research area SURG and by the Ministry of Health of the Czech Republic, grant No. NW26-04-00362.
Conflict of interest
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
Sources
1. Chovanec M, Zvěřina E, Kluh J et al. Zachování sluchu při mikrochirurgické léčbě vestibulárního schwannomu. Cesk Slov Neurol N 2015; 78/111 (4): 435–441.
2. Fík Z, Vlasák A, Čada Z et al. První zkušenosti s využitím přímé monitorace sluchového nervu u operací vestibulárního schwannomu v České republice. Cesk Slov Neurol N 2021; 84/117 (5): 477–480. doi: 10.48095/cccsnn2021477.
3. Zhan KY, Wick CC. Intraoperative cochlear nerve monitoring in vestibular schwannoma microsurgery. Otolaryngol Clin North Am 2023; 56 (3): 471–482. doi: 10.1016/j.otc.2023.02.007.
4. Watanabe N, Ishii T, Fujitsu K et al. Intraoperative cochlear nerve mapping with the mobile cochlear nerve compound action potential tracer in vestibular schwannoma surgery. J Neurosurg 2019; 130 (5): 1568–1575. doi: 10.3171/2017.12.JNS171545.
5. Miyazaki H, Caye-Thomasen P. Intraoperative auditory system monitoring. Adv Otorhinolaryngol 2018; 81 : 123–132. doi: 10.1159/000485577.
6. Jannetta PJ, Møller AR, Møller MB. Technique of hearing preservation in small acoustic neuromas. Ann Surg 1984; 200 (4): 513–523. doi: 10.1097/00000658-198410000-00012.
7. Fík Z, Chovanec M, Zvěřina E et al. Funkce lícního nervu po mikrochirurgické léčbě vestibulárního schwannomu. Cesk Slov Neurol N 2017; 80/112 (5): 545–551. doi: 10.14735/amcsnn2017545.
8. Behr R, Schwager K, Hofmann E. Auditory brainstem implants-hearing restoration in congenitally deaf children. Dtsch Arztebl Int 2022; 119 (9): 135–141. doi: 10.3238/arztebl.m2022.0090.
9. Zvĕrina E, Sollmann WP, Betka J et al. First auditory brainstem implant in the czech republic. J Laryngol Otol Suppl 2000; (27): 54–55. doi: 10.1258/0022215001904752.
10. Fik Z, Zverina E, Lisy J et al. Hearing after vestibular schwannoma surgery: is it preserved forever? Otol Neurotol 2023; 44 (3): 260–265. doi: 10.1097/MAO. 0000000000003801.
11. Lucas JC, Fan CJ, Jacob JT et al. Retrosigmoid approach for sporadic vestibular schwannoma: patient selection, technical pearls, and hearing results. Otolaryngol Clin North Am 2023; 56 (3): 509–520. doi: 10.1016/j.otc.2023.02.010.
12. Daher GS, Marinelli JP, van Gompel JJ et al. Congress of neurological surgeons systematic review and evidence-based guideline on hearing preservation outcomes in patients with sporadic vestibular schwannoma: update. Neurosurgery 2026; 98 (2): 298–302. doi: 10.1227/neu.0000000000003551.
13. Møller AR, Jannetta PJ. Auditory evoked potentials recorded from the cochlear nucleus and its vicinity in man. J Neurosurg 1983; 59 (6): 1013–1018. doi: 10.3171/jns.1983.59.6.1013.
14. Matthies C, Samii M. Direct brainstem recording of auditory evoked potentials during vestibular schwannoma resection: nuclear BAEP recording. technical note and preliminary results. J Neurosurg 1997; 86 (6): 1057–1062. doi: 10.3171/jns.1997.86.6.1057.
15. Nakatomi H, Miyazaki H, Tanaka M et al. Improved preservation of function during acoustic neuroma surgery. J Neurosurg 2015; 122 (1): 24–33. doi: 10.3171/2014.8.JNS132525.
16. Hosoya M, Nishiyama T, Wakabayashi T et al. Vestibular schwannoma surgery with endoscope-assisted retrolabyrinthine approach under modified reinforced continuous intraoperative monitoring for hearing preservation: experience of 33 cases in a single center. Diag-nostics (Basel) 2023; 13 (2): 275. doi: 10.3390/diagnostics13020275.
17. Sass HCR, Miyazaki H, West N et al. Extended retrolabyrinthine approach: results of hearing preservation surgery using a new system for continuous near real-time neuromonitoring in patients with growing vestibular schwannomas. Otol Neurotol 2019; 40 (5S Suppl 1): S72–S79. doi: 10.1097/MAO.0000000000002216.
18. Kuroki A, Møller AR. Microsurgical anatomy around the foramen of luschka in relation to intraoperative recording of auditory evoked potentials from the cochlear nuclei. J Neurosurg 1995; 82 (6): 933–939. doi: 10.3171/jns.1995.82.6.0933.
19. Ebinger K, Otto S, Arcaroli J et al. Multichannel auditory brainstem implant: US clinical trial results. J Laryngol Otol Suppl 2000; (27): 50–53. doi: 10.1258/0022215001904743.
20. Dastagirzada YM, Eremiev A, Wisoff JH et al. Auditory brainstem implantation: surgical experience and audiometric outcomes in the pediatric population. J Neurosurg Pediatr 2024; 33 (5): 496–504. doi: 10.3171/2023.12.PEDS23299.
Labels
Paediatric neurology Neurosurgery NeurologyArticle was published in
Czech and Slovak Neurology and Neurosurgery

2026 Issue 3
- Hope Awakens with Early Diagnosis of Parkinson's Disease Based on Skin Odor
- Advances in the Treatment of Myasthenia Gravis on the Horizon
- Deep stimulation of the globus pallidus improved clinical symptoms in a patient with refractory parkinsonism and genetic mutation
- Safety and Tolerance of Metamizole in Postoperative Analgesia in Children
Most read in this issue
- 100 years of the Czech Department of Neurology, Charles UniversityThe Henner school
- Intestinal pseudo-obstruction syndrome in a patient with acute polyradiculoneuritis
- Perinatal ischemic stroke – a review of current knowledge
- Epilepsy surgery in children operated on before 3 years of age – experience of the Motol epilepsy center