
Laparoskopická transpozice aberantních cév („vascular hitch“) u obstrukce pyeloureterální junkce – kazuistika
Laparoscopic transposition of crossing vessels („vascular hitch “) in ureteropelvic junction obstruction – a case report
Aim of the study: Crossing vessels of the lower renal pole are found in 10–15 % of children with ureteropelvic junction (UPJ) obstruction, and in more than half of older children and adolescents (2). The obstruction, caused by external pressure of the vessels on the UPJ or proximal ureter, is often intermittent and manifests by recurrent and even colic pain. In an acute condition, we can detect a high grade hydronephrosis that may disappear after resolution of the acute episode. The aim of this video is to show intraoperative evaluation and policy in hydronephrosis accompanied by crossing vessels and performance of laparoscopic repair without opening of the urinary tract according to Hellström (1).
Methods: Doppler ultrasound examination is of paramount importance in detection of crossing vessels of the lower renal pole. On intravenous urography, a globular shape of the pelvis with a flat bottom and calyceal dilatation has been described in crossing vessels (3). Surgery is considered in confirmed UPJ obstruction based on symptoms and findings on dynamic renal scintigraphy or on intravenous urography with furosemide. Functional magnetic resonance urography is a good alternative, moreover, detecting the crossing vessels (4) CT urography is inappropriate in children because of a high radiation burden.
If the vascular hitch is being considered, it should be born in mind, that an „extrinsic obstruction “, caused by external pressure of vessels or adhesions, may be accompanied by an „intrisic“ obstruction, a real UPJ or proximal ureter stenosis with pathohistological changes in the ureteric wall. In this case a dismembered repair should be performed (3).
Hellström described elevation and adventitial fixation of the vessels to the renal pelvis outside the region of UPJ in 1949 (1). Chapman proposed to stabilise the vessels in the new position by wrapping them in the pelvic wall. This method has gained popularity in selected patients especially after introduction of laparoscopy as an easier alternative to technically demanding laparoscopic suturing in dismembered pyeloplasty (5–7). The Chapman modification has been used in our case as well. Surgery has three phases. First, releasing of crossing vessels from the pelvis and ureter is performed and the vessels are freely pulled cranially outside the UPJ region. The second phase should prove free passage of urine after liquid infusion and furosemide administration. It is necessary to wait 10 minutes to achieve full diuretic effect. If UPJ obstruction persists at visual control, then a dismembered repair is to be used (8). During the third phase, the vessels are wrapped within the anterior pelvic wall at the elevated position according to Chapman.
Results and discussion: An 8-year-old boy was investigated because of intermittent abdominal pain. Grade II hydronephrosis of the right kidney with crossing vessels to the lower pole was detected on ultrasound and Doppler imaging. Diuretic scintigraphy with 99mTc-MAG3 has shown symmetrical differential renal function (48 %) and delayed drainage of the radionuclide pointing to a partial obstruction of the right kidney.
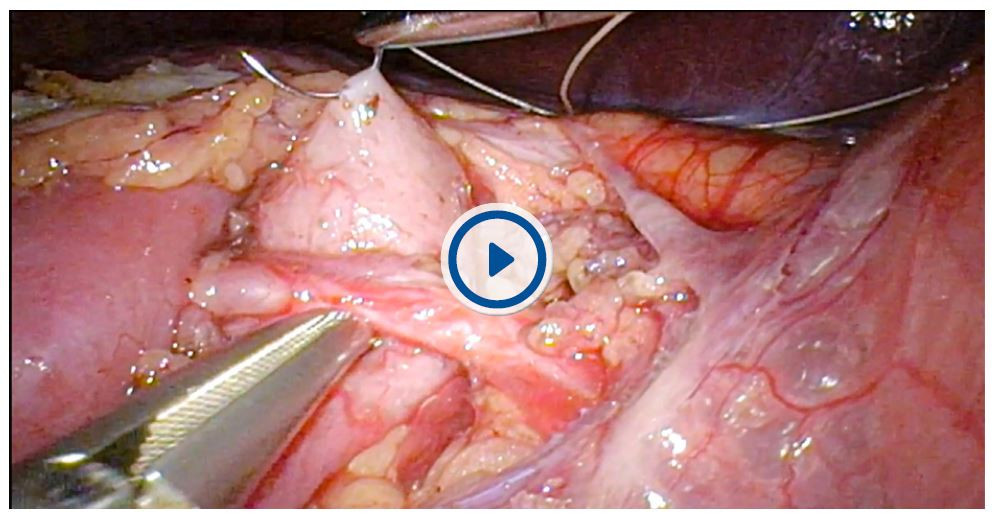
The right kidney was laparoscopically exposed in conventional transperitoneal way with three 5mm trocars inserted at umbilicus, above umbilicus in the midline and pararectal to umbilicus. The crossing vessels were released from the enlarged pelvis, UPJ and proximal ureter to enable free movement up and down behind the vessels („shoeshine manoeuvre “). After i.v. liquid infusion, the vessels were elevated from the UPJ region and 10 mg furosemide i.v. was administered. A good passage of urine from the pelvis to the ureter across the UPJ was confirmed. The vessels were wrapped into the pelvic wall well above the UPJ using two absorbable polyglactin 4/0 sutures. Length of surgery 115 min. Stenting was not necessary, therefore, no worry of stent syndrome and of necessity for additional anaesthesia to remove it. Postoperative course was uneventful, pain settled and dilatation of the pelvicalyceal system decreased at 3 - and 12 - months follow-up. Doppler imaging showed adequate cranial deflection of the crossing vessels and good perfusion of the kidney.
The laparoscopic vascular hitch was first published by Meng and Stoller in 2003 (6). Several articles have been published proving safety of the procedure. Its success rate (97,5 % ± 1,6 %) is comparable with dismembered pyeloplasty (9). The pros are: unstented repair, shorter length of surgery and hospital stay (9, 10).
Conclusions: Laparoscopic transposition of crossing vessels is a good alternative of dismembered pyeloplasty in selected patients with intermittent hydronephrosis once concomitant „intrinsic“ cause of UPJ obstruction has been excluded. It is a stent free procedure with a shorter operative time and shorter hospitalization.
Keywords:
hydronephrosis – ureteropelvic junction obstruction – UPJO – vascular hitch – transposition of renal crossing vessels
Autori:
Radim Kočvara; Josef Sedláček; Marcel Drlík
Pôsobisko autorov:
Urologická klinika VFN, Praha
Vyšlo v časopise:
Ces Urol 2021; 25(4): 231-235
Kategória:
Video
Súhrn
Cíl práce: Aberantní či křížící cévy (crossing vessels) k dolnímu pólu ledviny nalézáme u 10–15 % dětí s obstrukcí pyeloureterální junkce (PUJ), u starších dětí a dospívajích je to více než v polovině případů (2). Obstrukce vyvolaná tlakem cév na PUJ či subrenální močovod je často intermitentní a projevuje se opakovanou bolestí, až kolikovitého charakteru. V akutním stavu nacházíme výraznou hydronefrózu, která může po zklidnění vymizet. Cílem této videoprezentace je ukázka peroperační rozvahy při nálezu aberantních cév u hydronefrózy a technické provedení laparoskopické operace bez přerušení kontinuity močových cest podle Hellströma (1).
Metoda: Pro diagnostiku je klíčové Dopplerovské zobrazení samostatného svazku aberantních cév mířících k dolnímu pólu ledviny. Na vylučovací urografii se popisuje kulovitá intrarenální pánvička s plochým dolním okrajem a s dilatací kalichů (3). K operaci přistupujeme při prokázané obstrukci PUJ na základě symptomů a nálezu na dynamické scintigrafii ledvin či vylučovací urografii s furosemidem, alternativou je dynamická urografie magnetickou rezonancí, která navíc zřetelně zobrazí přítomnost aberantních cév (4). CT urografie je u dětí vzhledem k vysoké radiační zátěži zcela nevhodná.
Při rozhodování o provedení transpozice aberantních cév je třeba mít na paměti, že zevní „extrinzická“ obstrukce, způsobená zevním tlakem cévami či adhezemi, se může kombinovat s vlastní stenózou pyeloureterální junkce či subrenálního močovodu, tj. s „intrinzickou“ obstrukcí, při které nacházíme histologické změny ve stěně močovodu a kterou lze vyřešit pouze resekční pyeloplastikou (3).
Hellström popsal v r. 1949 vysunutí aberantních cév kraniálně mimo oblast PUJ s fixací cév za adventícii ke stěně pánvičky (1). Chapman navrhl fixovat cévy v nové poloze zanořením do stěny pánvičky a tato metoda doznala rozšíření zejména po zavedení laparoskopie jako jednodušší alternativa technicky náročnější resekční pyeloplastiky u vybraných pacientů (5–7). Také v našem případě jsme použili modifikaci podle Chapmana. Operace má tři fáze. První fází je uvolnění aberantních cév od stěny pánvičky a močovodu a jejich odtažení mimo oblast pyeloureterální junkce. Druhou fází je potvrzení dobré evakuace pánvičky při průběhu peristaltické vlny po zavodnění a podání furosemidu. Je třeba vyčkat plného efektu furosemidu nastupujícího po 10 min. od jeho podání. Pokud by vizuálně přetrvávala obstrukce PUJ, je nutné provést resekční pyeloplastiku (8). Třetí fází operace je zajištění cév ve vysunuté poloze modifikací dle Chapmana, tj. zanořením do přední stěny pánvičky.
Výsledky a diskuze: Prezentujeme případ osmiletého chlapce, který byl vyšetřován pro intermitentní bolesti břicha. Ultrazvukové vyšetření potvrdilo hydronefrózu II. stupně vpravo s nálezem aberantních cév k dolnímu pólu. Diuretická scintigrafie s 99mTc‑MAG3 ukázala dobrou separovanou funkci pravé ledviny (48 %) a částečnou obstrukci odtoku s opožděnou evakuací radiofarmaka. Laparoskopická operace se uskutečnila z klasického transperitoneálního přístupu se třemi 5mm trokary: v pupku, ve střední čáře nad pupkem a pararektálně vpravo od pupku. Svazek aberantních cév byl postupně zcela uvolněn od dilatované pánvičky, junkce a subrenálního močovodu, aby byl zajištěn volný pohyb pánvičky nahoru a dolů („shoeshine manoeuvre“). Při kraniálním vysunutí aberantních cév a po dostatečné hydrataci byl podán furosemid (10 mg i. v.) a potvrzena volná pasáž z pánvičky do močovodu. Cévy byly zanořeny dvěma vstřebatelnými stehy (polyglactin 4/0) do záhybu přední stěny pánvičky mimo oblast PUJ. Operace trvala 115 min. Při operaci není nutné zavádět stent. Vyhneme se tak stent syndromu a další celkové anestezii nutné k extrakci stentu u dítěte. Pooperační průběh byl bez komplikací, bolesti vymizely, dilatace kalichopánvičkového systému se s odstupem tří měsíců zmenšila a na Dopplerovském zobrazení je patrné příznivé kraniální vychýlení aberantní cévy a zachovalá perfuze dolního pólu ledviny.
Laparoskopickou transpozici aberantních cév, tzv. „vascular hitch“ poprvé popsali Meng a Stoller v r. 2003 (6). Od té doby vyšla řada prací potvrzujících bezpečnost provedení této operace. Její úspěšnost (97,5 % ± 1,6 %) je srovnatelná s resekční pyeloplastikou (9). Výhodou je bezstentová operace s kratší délkou operace a hospitalizace (9, 10).
Závěr: Laparoskopická transpozice aberantních cév je alternativou resekční pyeloplastiky u vybraných pacientů s intermitentní hydronefrózou, pokud při operaci vyloučíme současnou vlastní „intrinzickou“ obstrukci PUJ. Nevyžaduje inzerci stentu a zkracuje délku operace i hospitalizace.
Klíčová slova:
hydronefróza – obstrukce pyeloureterální junkce – vascular hitch – transpozice aberantních cév ledviny
Došlo: 16. 10. 2021
Přijato: 15. 11. 2021
Kontaktní adresa:
doc. MUDr. Radim Kočvara, CSc.
Urologická klinika VFN
Ke Karlovu 6
128 08 Praha 2
e-mail: radim.kocvara@vfn.cz
Střet zájmů: Žádný.
Prohlášení o podpoře: Podpořeno MZ ČR – RVO‑VFN64165.
Hlavní stanovisko: Předkládáme kazuistiku chlapce s obstrukcí pyeloureterální junkce způsobenou aberantními cévami, která byla vyřešena laparoskopickým vysunutím cév mimo oblast junkce podle Hellströma bez přerušení kontinuity močových cest (1). Podle našich informací, které bylo možné zjistit, nebyl tento způsob laparoskopické operace dosud v České republice publikován.
Major statement: This is a case report of a 8-year‑old boy with ureteropelvic junction (UPJ) obstruction caused by external pressure of lower renal pole crossing vessels. The obstruction has been resolved by laparoscopic elevation of the vessels out of the ureteropelvic junction according to Hellström, without opening of the urinary tract. (1) To the best of our knowledge, this type of laparoscopic procedure has not yet been published in the Czech Republic.
Zdroje
1. Hellström J, Giertz G, Lindblom K. Pathogenesis and treatment of hydronephrosis. In: Presentedat VIII Congreso de la Sociedad International de Urologia, Paris, France. 1949.
2. Cain MP, Rink RC, Thomas AC, et al. Symptomatic ureteropelvic junction obstruction in children in the era of prenatal sonography‑is there a higher incidence of crossing vessels? Urology 2001; 57(2): 338–341.
3. Menon P, Rao KLN, Sodhi KS, Bhattacharya A, et al. Hydronephrosis: Comparison of extrinsic vessel versus intrinsic ureteropelvic junction obstruction groups and a plea against the vascular hitch procedure J Pediatr Urol 2015; 11(2): 80.e1–e6.
4. Zerhau P, Kubátová J, Horák D, Skotáková J, Mach V. Použití magnetické rezonance v předoperačním posouzení obstrukce močového traktu u dětí. Rozhl Chir 2003; 82(2): 115–119.
5. Smith JS, McGeorge A, Abel BJ, Hutchinson AG. The results of lower polar renal vessel transposition (the Chapman procedure) in the management of hydronephrosis. Br J Urol 1982; 54(2): 95–97.
6. Meng MV, Stoller ML. Hellström technique revisited: laparoscopic management of ureteropelvic junction obstruction. Urology 2003; 62 : 404–408.
7. Villemagne T, Fourcade L, Camby C, et al. Long‑term results with the laparoscopic transposition of renal lower pole crossing vessels. J Pediatr Urol. 2015; 11(4): 174.e1–e7.
8. Esposito C, Bleve C, Escolino M, et al. Laparoscopic transposition of lower pole crossing vessels (vascular hitch) in children with pelviureteric junction obstruction. Transl Pediatr 2016; 5(4): 256–261.
9. Miscia ME, Lauriti G, Riccio A, et al. Minimally invasive vascular hitch to treat pediatric extrinsic ureteropelvic junction obstruction by crossing polar vessels: a systematic review and meta‑analysis. J Pediatr Urol 2021; 17(4): 493–501.
10. Kim JK, Keefe DT, Rickard M, et al. Vascular hitch for paediatric pelvi‑ureteric junction obstruction with crossing vessels: institutional analysis and systematic review with meta‑analysis. BJU Int. 2021; 19. doi: 10.1111/bju.15342.
Štítky
Detská urológia Nefrológia UrológiaČlánok vyšiel v časopise
Česká urologie
2021 Číslo 4
- Aktuálne európske odporúčania pre liečbu renálnej koliky v dôsledku urolitiázy
- MUDr. Šimon Kozák: V algeziológii nič nefunguje zázračne cez noc! Je dôležité nechať si poradiť od špecialistov
- Vyšetření T2:EGR a PCA3 v moči při záchytu agresivního karcinomu prostaty
- Lék v boji proti benigní hyperplazii prostaty nyní pod novým názvem Adafin
Najčítanejšie v tomto čísle
- Sérové onkomarkery karcinomu prostaty
- REZUM. Od prvního nápadu přes experiment a klinické studie až k běžné klinické praxi
- Poranění urogenitálního systému u dětí a adolescentů
- Liposarkom retroperitonea – kazuistika